
Things To Try for Persistent Acne Before Hopping on Accutane
A research-backed guide to addressing the root cause before resorting to Accutane

When I was dealing with acne, I did not fully understand what was causing it, and neither did the people I was paying to help me figure it out.
I tried everything that I saw online: benzoyl peroxide, salicylic acid, topical retinoids & antibiotics, a strict carnivore diet, and more than a thousand dollars in skincare products across different brands and formulations.
I was also seeing a dermatologist throughout this period, which turned out to be both a waste of time and money.
When I asked the lead dermatologist whether eating certain foods like pizza could cause breakouts, he told me that food had no effect on acne whatsoever, and that the only way pizza would ever cause a breakout is if I picked it up and rubbed it directly on my face.
I eventually went on Accutane, which cleared my skin after about seven months of use, but the first couple of months involved a purging phase where my acne was more than twice as bad as it had ever been.
The side effects throughout the course were significant:
Hair loss
Skyrocketed cholesterol
No libido
Joint pain
Persistent facial puffiness
Depression
Each time I raised one of these with the clinic, I was told they would improve over time, which was not the case.
Accutane is a synthetic retinoid (a derivative of vitamin A) that works by reducing sebum production, shrinking the sebaceous glands, and slowing the turnover of cells lining the follicle.
While it is effective, it carries significant risk that a large number of people online describe as having seriously damaged their health in ways that outlasted the course itself.
In many cases the effects appear to be persistent in a way that is comparable to post-finasteride syndrome, where a subset of users report lasting hormonal, neurological, and sexual dysfunction long after discontinuing the drug.
My acne also returned a few months after stopping the drug, which made it clear that Accutane had not addressed whatever was actually causing it.


Working out what that was, and addressing it directly, is what eventually resolved the problem, and this article covers what I found along the way.
What Causes Acne
The standard explanation for acne is that it is an androgenic condition.
Excess testosterone and DHT stimulate the sebaceous glands, producing excess sebum, clogged follicles, bacterial colonization, and inflammation. This framing has driven most conventional acne treatments for decades, and is probably wrong, or at least significantly incomplete.
Acne is better understood as an inflammatory condition driven primarily by gut dysfunction and the hormonal dysregulation that follows.
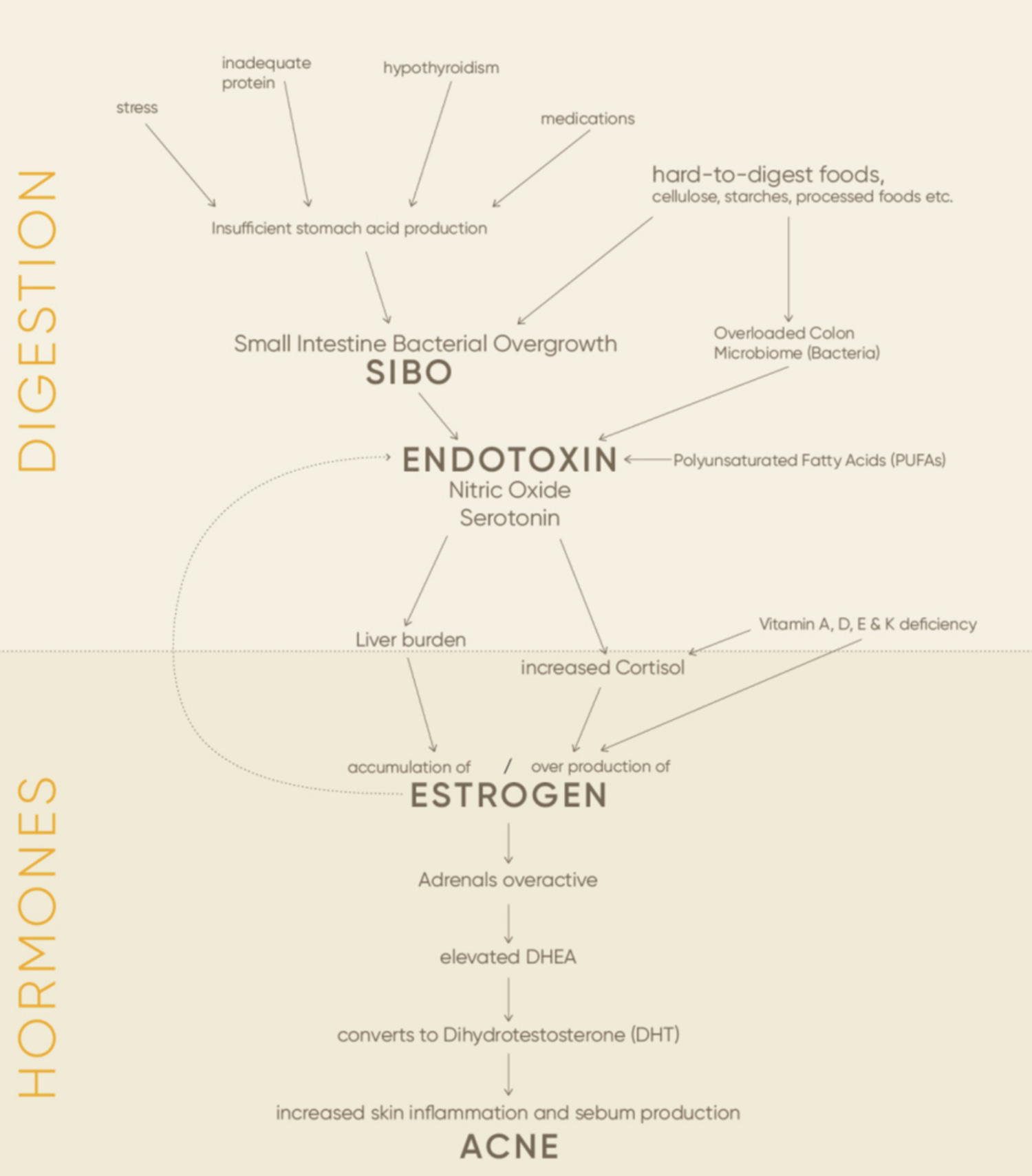
The gut is the body’s primary line of defense against bacterial toxins.
Gram-negative bacteria, which make up a large portion of the gut’s microbial population, release a compound called endotoxin when they die. Under normal conditions, the intestinal barrier prevents this from entering circulation, but in a large number of people this barrier is not functioning as it should.
Small intestinal bacterial overgrowth (SIBO) is part of the reason why.
When bacterial populations accumulate in the small intestine, which should contain very little bacteria, the endotoxin produced passes directly into circulation rather than being contained and cleared.
SIBO increases intestinal permeability and allows endotoxin to translocate into the bloodstream. [1]
Several things contribute to this:
Low stomach acid, which is the primary mechanism keeping bacteria confined to the colon
A poorly functioning ileocecal valve, which normally prevents colonic bacteria from migrating back into the small intestine
A gut barrier that has been progressively weakened by chronic exposure to endotoxin, serotonin, and nitric oxide
Circulating endotoxin places a significant burden on the liver, which is responsible for the clearance and detoxification of gut-derived endotoxin.
Chronic endotoxin load impairs this process, allowing toxic levels to develop in liver tissue and enter systemic circulation. [2]
The liver is also the primary site of estrogen detoxification through glucuronidation and sulfation. When it is overburdened by endotoxin, estrogen clearance is compromised and estrogen accumulates.
At the same time, endotoxin directly activates the adrenal gland, raising cortisol and increasing estrogen synthesis further.
Elevated estrogen is a direct contributor to acne.
Estrogen receptors are expressed in the sebaceous glands, and excess estrogen keeps the adrenal glands chronically overactive. Estrogen also sensitizes hepatic Kupffer cells to endotoxin, amplifying the inflammatory response and compounding the burden on the liver. [3]
The skin is one of the earliest and most visible indicators of the state of the gut.
Inflammatory lesions tend to appear first on the face and neck, and spread to the back, chest, and torso as the underlying condition becomes more severe. This pattern maps directly onto the severity of the endotoxin load, and is not consistent with a purely androgenic explanation.
This is where the androgen theory loses its validity.
Tetracycline antibiotics (e.g. doxycycline, minocycline) are routinely prescribed for hormonal acne, and they are known to lower estrogen while simultaneously raising DHT levels. If androgens were the primary driver, these drugs would worsen acne, but they do not. I have also applied DHT topically to my face without any breakouts, and if anything my skin appeared clearer during that period.
Published research supports this.
A study of 90 women with acne found no correlation between androgen levels and acne severity. [4]
A separate study concluded that the role of androgens in acne is permissive rather than causative, and that plasma androgen measurements have no place in its clinical management. [5]
For a more detailed treatment of this subject, the article that was most important in shaping my understanding of it can be found here:
Skin Breakouts Broken Down With Georgi Dinkov
I am not a doctor. None of this is medical device. It reflects my personal experience and research. Do your own research and due diligence before trying anything discussed here.
Diet and Food-Based Interventions
Daily Insoluble Fiber
Insoluble fiber—which is found in raw carrots, bamboo shoots, and white button mushrooms—passes through the digestive tract largely undigested, sweeping the intestinal walls and reducing bacterial load and endotoxin accumulation.
Raw carrots are particularly useful.
They contain a unique combination of insoluble fiber and natural antibacterial compounds, including falcarinol, that discourage bacterial overgrowth in the small intestine. The fiber also binds to excess estrogen and endotoxin in the digestive tract, carrying them out before they can be reabsorbed.
A daily raw carrot—grated lengthwise, with a small amount of olive oil and vinegar—is an effective intervention for acne. White button mushrooms prepared the same way serve a similar purpose and can be rotated in or used alongside it.
As covered in my recent article (A Non-Exhaustive List of My Favorite Biohacks), white button mushrooms show the strongest dose-dependent inhibition of aromatase among all vegetables tested, which directly addresses estrogen excess.
Olive oil increases the antibacterial effect and improves absorption of fat-soluble compounds. Vinegar contributes additional antimicrobial activity.
Weekly Oysters
Acne patients consistently show lower serum zinc levels than healthy controls, and zinc supplementation has been shown to reduce both inflammatory and non-inflammatory acne lesions. [6]
Zinc has a bacteriostatic effect on Cutibacterium acnes, inhibits chemotaxis, and reduces the production of inflammatory cytokines. [7]
It is also required for the synthesis of retinol-binding protein—the carrier that delivers vitamin A to the skin. Acne patients have been shown to have lower retinol-binding protein levels than those with mild acne or healthy controls. [8]
Without sufficient zinc, vitamin A cannot reach the tissue that needs it regardless of dietary intake.
Oysters are the single richest food source of zinc, containing ~74mg per serving.
 : Grocery & Gourmet Food")
Eating a can of oysters in olive oil once or twice per week is enough to meaningfully support zinc status without relying on supplementation. They are also a good source of selenium, copper, and vitamin B12.
Sufficient Vitamin C
Vitamin C is an essential cofactor for collagen synthesis, directly activating the transcription factors involved in collagen production and stabilizing procollagen mRNA. [9]
In the context of acne, this matters for two reasons.
Active lesions involve tissue damage that requires collagen for repair, and the post-inflammatory scarring that follows is determined in large part by how efficiently that repair occurs.
Vitamin C also functions as a primary antioxidant in the skin, reducing oxidative damage from UV radiation and environmental stress.
Dietary sources including oranges, guava, and kiwi are preferable to supplementation where possible, as whole food sources come with synergistic cofactors.
Replace A1 Dairy w/A2 or Eggshell Calcium
Most commercial dairy comes from cows that produce A1 beta-casein.
When digested, A1 beta-casein releases a peptide called beta-casomorphin-7 (BCM-7), which has been shown to induce pro-inflammatory immune activation and increase gut dysfunction.
A2 beta-casein does not generate this fragment. [10]
A systematic review found that consumption of milk containing A1 beta-casein was associated with increased gastrointestinal inflammation and delayed transit compared to milk containing only A2 beta-casein. [10]
A meta-analysis of over 78,000 children, adolescents, and young adults found that dairy consumption was associated with a significantly increased risk of acne across all forms (e.g. milk, cheese, yogurt) with the association strongest for low-fat and skim milk. [11]
Switching to A2 dairy where available, or removing dairy entirely and replacing calcium intake through eggshell calcium, removes this source of gut irritation without sacrificing nutrient density.
High-Dose Vitamin A or Beef Liver
Vitamin A is directly involved in the regulation of sebum production and the differentiation of the epithelial cells lining the follicle.
Deficiency leads to keratinization disorders, follicular plugging, and impaired skin cell turnover—all of which contribute directly to acne pathogenesis. [12]
Accutane itself is a synthetic retinoid that works by flooding this system at a pharmacological dose.
Before isotretinoin was approved in 1982, high-dose vitamin A was the standard treatment for severe acne.


A review of eight clinical trials conducted between the 1940s and 1980s found that acne improved in all but one, with 100,000 IU per day being the most commonly used and successful dose. Mean time to clinical improvement ranged from seven weeks to four months, which is comparable to isotretinoin. [13]
Getting sufficient dietary vitamin A through liver, egg yolks, and full-fat dairy addresses the same pathway at a physiological level. High-dose vitamin A is not without side effects, but the risk profile is much more favorable than Accutane.
Supplements
High-Dose Pantothenic Acid (Vitamin B5)
Pantothenic acid is a component of coenzyme A (CoA), which plays a central role in fatty acid metabolism.
The proposed mechanism for its effect on acne is that insufficient CoA availability causes the body to prioritize hormone production over fatty acid metabolism in the sebaceous glands, resulting in excess sebum accumulation and acne.
High-dose supplementation provides enough pantothenic acid to support both processes simultaneously. [14]

A randomized, double-blind, placebo-controlled trial of 41 adults with mild to moderate acne found that pantothenic acid supplementation significantly reduced total lesion count, inflammatory lesion count, and quality-of-life scores at 12 weeks compared to placebo. The supplement was well tolerated with no significant adverse effects. [15]
The doses used in clinical research range from 2.2g to 10g per day.
Starting low and titrating up is advisable. High doses can cause loose stools, which is a reliable indicator that the upper limit has been reached. It is also worth noting that pantothenic acid and biotin share the same intestinal transporter—the sodium-dependent multivitamin transporter (SMVT)—meaning that high doses of either can competitively inhibit the absorption of the other. [16]
Keep this in mind when supplementing with high doses of pantothenic acid over an extended period of time.
Daily Low-Dose Aspirin
Aspirin is useful in this context for two reasons.
The first is its anti-estrogenic effect. Aspirin inhibits COX-2, which suppresses aromatase activity—the enzyme responsible for converting androgens into estrogen.
A double-blind, placebo-controlled trial found that 100 mg of aspirin daily for six weeks produced a significant 23% reduction in estradiol levels. [17]
The second is its antimicrobial effect on the small intestine. Aspirin is absorbed primarily in the stomach and small intestine, which makes it an effective agent against SIBO before it reaches the colon.
A dose of 81 to 325 mg taken with food is sufficient. Since aspirin inhibits platelet aggregation, pairing it with vitamin K2 helps maintain normal clotting function and reduces the risk of excess bleeding.
CamphoSal + Activated Charcoal + Coconut Oil
This combination targets the colon directly, which aspirin can not reach on its own.
Camphor and phenyl salicylate (CamphoSal) work similarly to rifaximin—a non-absorbable antibiotic used for SIBO—in that they are not absorbed in the upper digestive tract and reach the colon intact where they exert an antimicrobial effect.
Activated charcoal binds endotoxin and other bacterial metabolites, preventing their absorption into circulation.
Coconut oil contributes additional antibacterial activity and, when combined with charcoal, is carried further down the digestive tract than it would be if taken alone.



Together they address the colonic bacterial load and endotoxin accumulation that drive the hormonal cascade described earlier. This combination does not need to be used daily. Two to three times per week is sufficient for most people.
Topical Treatments
Vitamin E Spot Treatment
Vitamin E applied topically to an active lesion reduces inflammation through several direct mechanisms.
Alpha-tocopherol inhibits COX-2 expression and iNOS in skin cells, which decreases prostaglandin E2 synthesis and nitric oxide production—two primary mediators of the redness and swelling associated with an acne breakout. [18, 19]
It also decreases the release of pro-inflammatory cytokines including IL-1β, IL-6, and TNF-α. [20]
As a fat-soluble antioxidant, it integrates into cell membranes and protects them from the lipid peroxidation that drives oxidative damage during the inflammatory phase.
Acne patients consistently show lower vitamin E levels in both serum and sebum than healthy controls, which means the tissue most affected by active lesions is also the most depleted of the compound that would normally protect it. [21]
For post-inflammatory hyperpigmentation, beta, gamma, and delta tocopherols have been shown to directly inhibit tyrosinase and reduce melanin production in cell models—reducing the dark marks that follow a breakout. [22]
I apply it directly to acne lesions before bed and consistently notice it looking less inflamed by morning.
For this purpose, a mixed tocopherol product—containing alpha, beta, gamma, and delta forms—is more effective than pure alpha-tocopherol alone, as the other forms contribute more directly to both COX-2 inhibition and tyrosinase suppression.
SkinFood’s vitamin E product (E Complete) is my preferred source.
TocoVit from IdeaLabs is another good option.
Baking Soda Face Wash
This one is based primarily on personal experience.
Rubbing a small amount of baking soda on the face and washing it off has consistently made my skin look less red and less inflamed.
There is some research basis for the antimicrobial properties of sodium bicarbonate.
It has demonstrated inhibitory activity against bacterial and fungal species responsible for skin infections in vitro, and a dermatology review concluded it may be an effective and safe dermatological agent in several capacities. [23]
However, a randomized controlled study on topical sodium bicarbonate in psoriasis found no reduction in erythema, and no human studies have examined its use specifically for acne. [24]
Regardless, I have had only positive experiences with it.
Avoid Commercial Skincare Products
Most commercial skincare products, including those marketed specifically for acne, contain preservatives and stabilizers with documented endocrine-disrupting properties.
Parabens, the most common preservatives in liquid skincare products, are readily absorbed through the skin and have been shown to mimic estrogen in tissue. [25]
Phthalates, found in fragrances and plasticizers, have been linked to altered testosterone and reproductive hormone changes in human studies. [26]
Chemical UV filters such as oxybenzone have shown estrogenic activity in laboratory studies and measurable skin absorption in humans. [27]
The simplest approach to circumvent this problem is to reduce product count to the minimum necessary. Water, a gentle cleanser, targeted spot treatments, and clean lotions are more than enough.
Light & Peptide Therapy
Red Light Therapy
Red light therapy, or photobiomodulation, uses low-level light in the 620 to 850 nm range to alter biological processes in skin cells without generating heat. In the context of acne, it works through two primary mechanisms.
The first is anti-inflammatory.
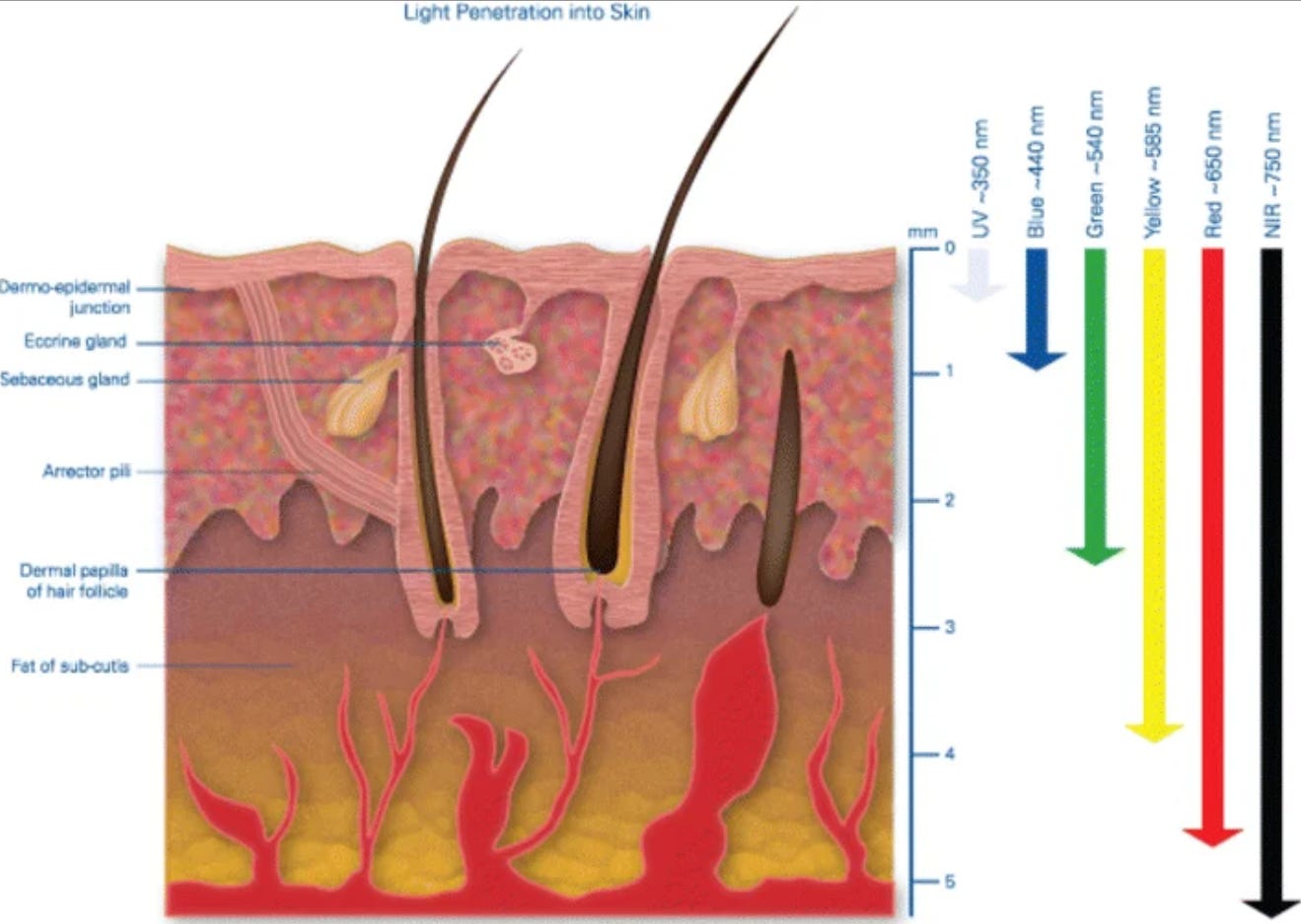
Red light penetrates deep enough to reach the sebaceous glands, where it reduces lipid production, modulates cytokine release from macrophages, and downregulates the inflammatory signaling that drives active lesions. [28]
A review of visible light in acne treatment confirmed that red light in the 620 to 750 nm range has well-documented anti-inflammatory effects with good skin penetration, including to the level of the sebaceous gland. [29]
The second is tissue repair.
Red light stimulates fibroblast activity and collagen synthesis, which directly supports the resolution of post-inflammatory lesions and reduces the likelihood of scar formation.
This makes it useful both during an active breakout and in the recovery phase.
A clinical study involving 35 participants found that daily red and blue LED therapy for four weeks reduced inflammatory acne lesions by 77% and non-inflammatory lesions by 54%, with pathological results confirming reduced sebaceous secretion, reduced inflammatory cell infiltration, and decreased sebaceous gland size. [30]
Ten to twenty minutes per day, three to five times per week, is the range used in most clinical protocols.
GHK-Cu Copper Peptide
GHK-Cu (glycyl-L-histidyl-L-lysine-copper) is a naturally occurring tripeptide found in human plasma, saliva, and urine.
Levels are around 200 ng/ml at age 20 and decline to roughly 80 ng/ml by age 60. This decline coincides with a measurable reduction in tissue regenerative capacity. [31]
In the context of acne, its relevance is primarily post-inflammatory.
Active lesions cause tissue damage that requires collagen synthesis, fibroblast migration, angiogenesis, and extracellular matrix remodeling for proper repair.
GHK-Cu has been shown to stimulate all of these processes. [31, 32]
It also reduces TNF-alpha induced secretion of the pro-inflammatory cytokine IL-6 in normal human dermal fibroblasts, an effect significant enough that the authors of one study proposed it as a topical alternative to corticosteroids in inflammatory skin conditions. [32]
Applied topically to active lesions or areas of post-inflammatory hyperpigmentation, it accelerates tissue repair and reduces the inflammatory environment that prolongs healing.
The research on it is largely preclinical and in vitro, with limited human RCTs, but the mechanistic basis is well established and the safety profile is favorable. [33]
Antibiotics
Minocycline / Doxycycline / Penicillin
When the gut bacterial burden is significant enough that diet and other interventions are not moving the needle, antibiotics become worth considering.
The conventional explanation for why antibiotics work is that they reduce C. acnes on the skin. The more probable explanation is that they reduce bacterial load and endotoxin in the gut, which is where the hormonal dysregulation driving the acne originates.
Reducing that load lowers the burden on the liver, reduces circulating endotoxin, and gives the body the conditions it needs to regulate estrogen properly.
Tetracycline antibiotics, particularly minocycline and doxycycline, are the most studied in this context.
Beyond their antimicrobial activity, both have well-documented immunomodulatory properties that operate independently of bacterial killing.
Minocycline inhibits pro-inflammatory enzymes including iNOS, MMPs, and COX-2, suppresses inflammatory cytokines including IL-1β, IL-6, IL-8, and TNF-α, and restores epithelial barrier integrity in colitis models. [34, 35]
It has also been shown to reduce intestinal bacterial load and modulate gut microbiota composition, which directly addresses the SIBO-driven endotoxin accumulation at the root of hormonal acne. [36]
The estrogen-lowering effect of tetracyclines is a separate and clinically relevant mechanism.
Tetracyclines reduce enterohepatic recirculation of estrogen by altering the gut bacteria responsible for deconjugating estrogen metabolites in the bile, reducing the reabsorption of free estrogen back into circulation and lowering systemic estrogen levels. [37]
This is why tetracyclines are known to reduce the efficacy of estrogen-based oral contraceptives, and it is also part of why they work for hormonal acne.
Minocycline has a favorable safety profile at doses up to 200 mg per day, with common side effects limited to light-headedness, vestibular symptoms, and nausea at standard doses. Most are dose-dependent and resolve quickly on discontinuation. [38]
Penicillin is worth mentioning separately.
Unlike broad-spectrum tetracyclines, penicillin acts primarily on gram-positive bacteria and has a narrower disruption profile on the overall gut microbiome.
In the context of acne, this makes it a useful option for targeting specific bacterial populations without the broader microbiome disruption that comes with long-term tetracycline use.
Antibiotics should not be approached carelessly.
There is enough anecdotal data and scientific evidence to take the side effect profile seriously, particularly with extended use. Starting at the smallest measurable dose and titrating up slowly is essential. Supplementing with a generous amount of vitamin K2 throughout any course is something I consider non-negotiable, as is closely monitoring symptoms and adjusting accordingly.
Conclusion
The interventions on this list are not a substitute for addressing the root cause. Cleaning up the diet, fixing digestion, and reducing endotoxin load will do more for persistent acne than any supplement or topical treatment.
If you have done all of that and are still struggling, the interventions covered here can meaningfully accelerate the process. None of them are quick fixes, but they address real mechanisms rather than masking symptoms.
References
[1] Losurdo et al. (2020), The Influence of Small Intestinal Bacterial Overgrowth in Digestive and Extra-Intestinal Disorders
[2] Nolan (1975), The role of endotoxin in liver injury
[3] Ikejima et al. (1998), Estrogen increases sensitivity of hepatic Kupffer cells to endotoxin
[4] Cibula et al. (2000), The role of androgens in determining acne severity in adult women
[5] Levell et al. (1989), Acne is not associated with abnormal plasma androgens
[6] Yee et al. (2020), Serum zinc levels and efficacy of zinc treatment in acne vulgaris: A systematic review and meta-analysis
[7] Cervantes et al. (2018), The Role of Zinc in the Treatment of Acne: A Review of the Literature
[8] Michaëlsson, Vahlquist & Juhlin (1977), Serum zinc and retinol-binding protein in acne
[9] Pullar, Carr & Vissers (2017), The Roles of Vitamin C in Skin Health
[10] Brooke-Taylor et al. (2017), Systematic Review of the Gastrointestinal Effects of A1 Compared with A2 β-Casein
[11] Juhl et al. (2018), Dairy Intake and Acne Vulgaris: A Systematic Review and Meta-Analysis of 78,529 Children, Adolescents, and Young Adults
[12] Everts (2012), Endogenous retinoids in the hair follicle and sebaceous gland
[13] Cook et al. (2022), Oral vitamin A for acne management: a possible substitute for isotretinoin
[14] Leung (1995), Pantothenic acid deficiency as the pathogenesis of acne vulgaris
[15] Yang et al. (2014), A Randomized, Double-Blind, Placebo-Controlled Study of a Novel Pantothenic Acid-Based Dietary Supplement in Subjects with Mild to Moderate Facial Acne
[16] Said (2009), Cell and molecular aspects of human intestinal biotin absorption
[17] Mohamadi et al. (2022), Aspirin versus placebo on estrogen levels in postmenopausal women: a double-blind randomized controlled clinical trial
[18] Yoshida et al. (2006), Topical application of a novel, hydrophilic gamma-tocopherol derivative reduces photo-inflammation in mice skin
[19] Wu et al. (2008), IL-8 production and AP-1 transactivation induced by UVA in human keratinocytes: roles of D-alpha-tocopherol
[20] Singh & Jialal (2004), Anti-inflammatory effects of alpha-tocopherol
[21] Ozuguz et al. (2014), Evaluation of serum vitamins A and E and zinc levels according to the severity of acne vulgaris
[22] Kamei et al. (2009), Comparison of the inhibitory effects of vitamin E analogues on melanogenesis in mouse B16 melanoma cells
[23] Rosenberg et al. (2024), Baking Soda and the Skin: A Review of Baking Soda in Dermatology
[24] Mazzarello et al. (2019), Efficacy of a Topical Formulation of Sodium Bicarbonate in Mild to Moderate Stable Plaque Psoriasis: a Randomized, Blinded, Intrapatient, Controlled Study
[25] Darbre & Harvey (2008), Paraben esters: review of recent studies of endocrine toxicity, absorption, esterase and human exposure
[26] Jurewicz & Hanke (2011), Exposure to phthalates: reproductive outcome and children health
[27] Matta et al. (2019), Effect of Sunscreen Application Under Maximal Use Conditions on Plasma Concentration of Sunscreen Active Ingredients
[28] Guo et al. (2025), The Application of Light Emitting Diode (LED) in Cosmetic Dermatology
[29] Akuffo-Addo et al. (2024), Visible Light in the Treatment of Acne Vulgaris
[30] Kwon et al. (2013), The clinical and histological effect of home-use, combination blue-red LED phototherapy for mild-to-moderate acne vulgaris in Korean patients: a double-blind, randomized controlled trial
[31] Pickart (2008), The human tri-peptide GHK and tissue remodeling
[32] Pickart et al. (2015), GHK Peptide as a Natural Modulator of Multiple Cellular Pathways in Skin Regeneration
[33] Wojcieszuk et al. (2025), BPC-157 and GHK-Cu in Wound Healing and Tissue Repair: A Review of Clinical Efficacy and Safety
[34] Garrido-Mesa, Zarzuelo & Gálvez (2013), Minocycline: far beyond an antibiotic
[35] Garrido-Mesa et al. (2011), The intestinal anti-inflammatory effect of minocycline in experimental colitis involves both its immunomodulatory and antimicrobial properties
[36] Vezza et al. (2022), Minocycline Prevents the Development of Key Features of Inflammation and Pain in DSS-induced Colitis in Mice
[37] Kwa et al. (2016), The Intestinal Microbiome and Estrogen Receptor–Positive Female Breast Cancer
[38] Gump et al. (1977), Side effects of minocycline: different dosage regimens
Great article, really enjoyed reading.
Great article very well written