
The 10 Most Fascinating Research Papers I Have Ever Come Across
1) Testosterone administration reduces lying in men

I have spent the last couple of years reading scientific literature to develop a better understanding of the human body and to access information directly rather than relying on someone else’s interpretation.
Along the way, I have come across a large number of research papers that have surprised me, challenged what I thought I knew, or simply made me think differently about something.
These are the ten that I found most interesting:
Testosterone administration reduces lying in men
Avoidance of sun exposure is a risk factor for all-cause mortality
A wandering mind is an unhappy mind
The serotonin theory of depression: a systematic umbrella review of the evidence
Minocycline, a microglial inhibitor, reduces ‘honey trap’ risk in human economic exchange
Progress on mitochondria and hair follicle development in androgenic alopecia
The tenacious brain: how the anterior mid-cingulate contributes to achieving goals
Refined carbohydrate consumption and facial attractiveness
Meal timing trajectories in older adults and their associations with morbidity, genetic profiles, and mortality
Emotional suppression and mortality risk over a 12-year follow-up
For each paper, I have outlined the study design, the primary findings, and what the data actually shows.
1) Testosterone administration reduces lying in men
Type of study: Double-blind, placebo-controlled trial
Sample size: 91 healthy young men
Duration: 2 days
Intervention: 50 mg transdermal testosterone gel vs. placebo
Key finding: Testosterone administration significantly reduced self-serving lying behavior
This study investigated whether testosterone has a causal effect on dishonest behavior in men. Prior research had established correlations between testosterone levels and various social behaviors, but most of that evidence was observational. This paper aimed to establish causation using a controlled experimental design.
91 healthy young men participated in a double-blind, placebo-controlled trial conducted over two consecutive days. On day one, subjects were randomly assigned to receive either 50 mg of Testogel (a transdermal testosterone gel) or a placebo gel applied to the upper right arm. The testosterone was allowed to absorb for 21 to 24 hours before any behavioral tasks were administered. On day two, subjects completed a die-rolling task and a post-experiment questionnaire, after which a blood sample was taken to verify testosterone levels.
The die-rolling task worked as follows. Each subject rolled a six-sided die in private and self-reported the result into a computer. The payout was equal to the number reported in euros for rolls of one through five, and zero euros for a six. Because only the self-reported number was recorded, and not the actual roll, subjects had a clear financial incentive to lie, and no risk of being caught doing so individually. Lying could only be detected at the group level by comparing the distribution of reported outcomes to what a fair die would be expected to produce.
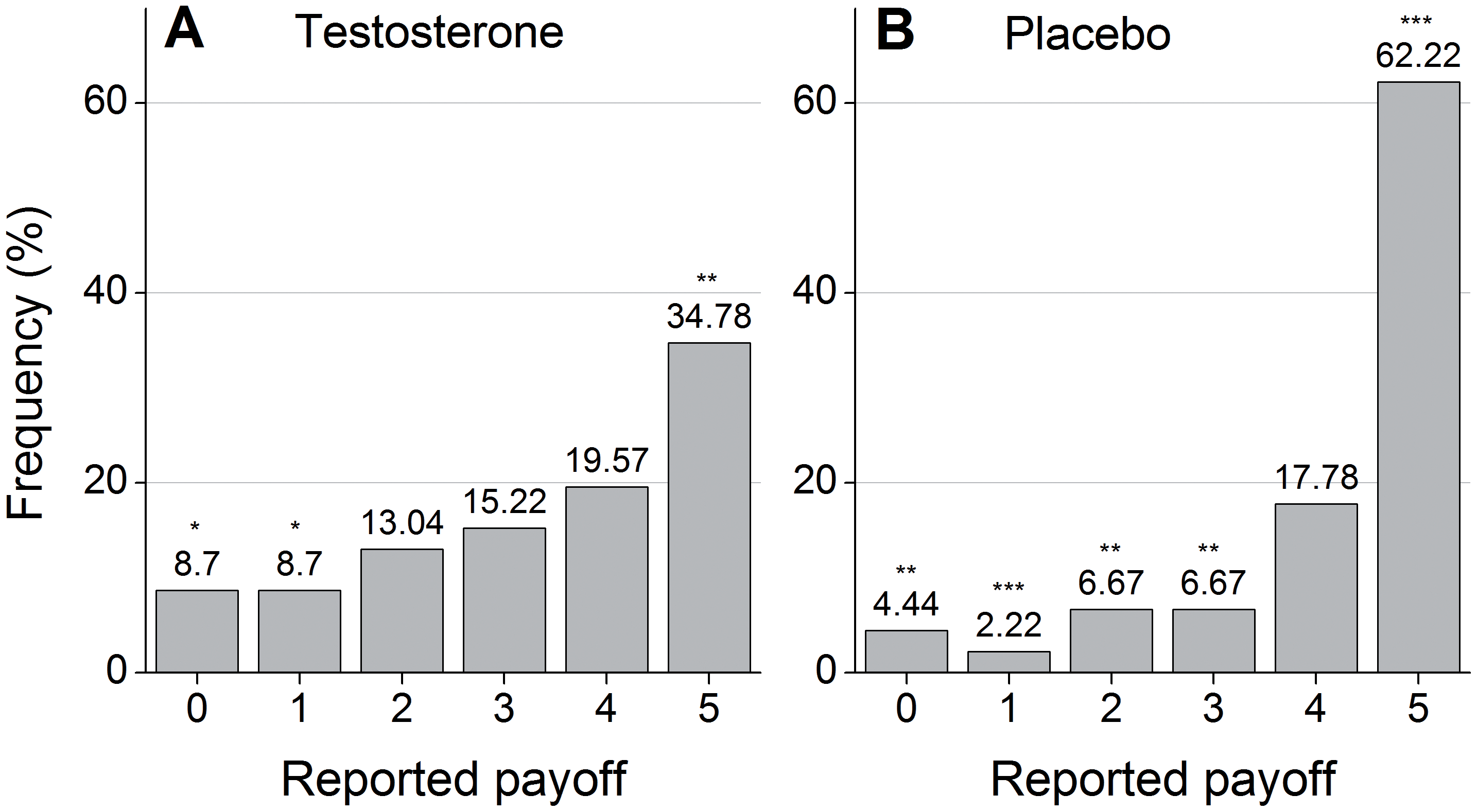
The placebo group reported an average payoff of 4.18 euros. The testosterone group reported an average of 3.33 euros. This difference was statistically significant (p = 0.005). The gap was most pronounced at the highest-value outcome: 62.2% of placebo subjects reported a roll of five, compared to 34.8% of testosterone subjects—a result that was also statistically significant (p = 0.012). Both groups lied more than chance would predict, but the testosterone group lied substantially less.
A correlation analysis across the full sample found that higher testosterone levels were associated with lower reported payoffs (Pearson’s r = −0.22, p = 0.035), meaning the relationship held not just between groups but within the pooled data as well. OLS regressions confirmed the treatment effect was robust after controlling for age, personality variables including the Big Five and Machiavellianism, and economic preference measures including risk tolerance, impulsivity, and reciprocity.
One concern with placebo-controlled hormone studies is that subjects may guess which condition they are in and adjust their behavior accordingly. The researchers addressed this directly. Among the subsample asked, there was no correlation between actual and perceived testosterone administration (p = 0.94), and subjects who believed they had received testosterone did not report higher payoffs than those who believed they had received placebo (p = 0.179). A pure expectation effect is therefore unlikely to explain the results.
The authors propose two main interpretations. The first is that testosterone directly increases prosocial preferences—in this case, honesty. The second is that testosterone heightens status concerns and pride, making dishonest behavior feel dishonorable even when undetectable. This second interpretation is consistent with prior work suggesting testosterone motivates dominance-seeking behavior, which in certain contexts expresses itself as prosocial rather than aggressive conduct. The researchers could not distinguish between these two mechanisms.
2) Avoidance of sun exposure is a risk factor for all-cause mortality
Type of study: Prospective cohort study
Sample size: 29,518 women
Duration: 20 years (1990–2011)
Population: Swedish-born women aged 25–64
Key finding: Avoiding sun exposure was associated with a twofold increase in all-cause mortality
Most public health messaging around sun exposure has focused on its risks—primarily skin cancer, and melanoma in particular. This study took the opposite angle, asking whether avoiding sun exposure carries its own mortality risk. It is one of the few large-scale longitudinal studies to treat sun avoidance as an independent risk factor rather than a protective behavior.
The data came from the Melanoma in Southern Sweden (MISS) cohort, initiated in 1990. Approximately 30,000 Swedish-born women between the ages of 25 and 64 were recruited from the general population registry of South Sweden, representing around 20% of women in those age groups in the region. At enrollment, participants completed a detailed questionnaire covering sun exposure habits, smoking, alcohol consumption, marital status, education level, income, BMI, physical exercise, and number of pregnancies. A follow-up questionnaire was administered between 2000 and 2002. Deaths and cancer diagnoses were tracked through the National Cancer Register, the Cause of Death Register, and the National Population Register up to January 2011.
Sun exposure was assessed using four questions: how often subjects sunbathed in summer, whether they sunbathed during winter holidays, how often they used tanning beds, and whether they traveled abroad to swim and sunbathe. Each question was coded as yes or no, and a composite score from zero to four was created based on the number of affirmative answers. Women who answered no to all four questions were classified as sun avoiders and used as the reference group.
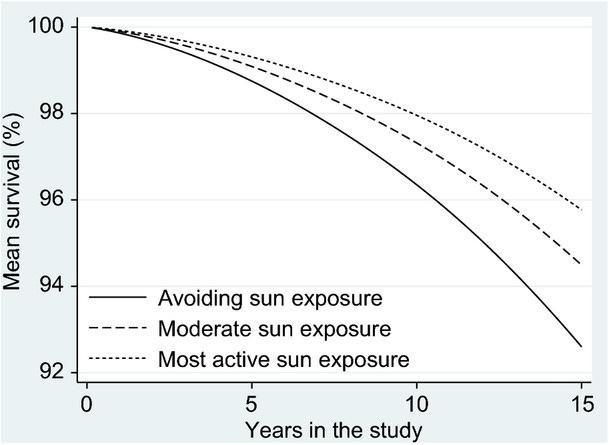
There were 2,545 deaths across 540,577 person-years of follow-up. The relationship between sun exposure and all-cause mortality followed a clear dose-dependent pattern. Compared to women with the highest sun exposure, those who avoided sun entirely had double the mortality rate (HR 2.0, 95% CI 1.6–2.5). Those with moderate exposure had a 40% higher mortality rate (HR 1.4, 95% CI 1.1–1.7). This gradient held after adjusting for age, smoking, education, income, marital status, comorbidity, BMI, and physical exercise.
One of the more striking findings involved the comparison between sun avoiders and smokers. Nonsmokers who avoided sun exposure had a similar life expectancy to smokers with the highest sun exposure. The authors concluded that sun avoidance appeared to carry a mortality risk of comparable magnitude to smoking in terms of life expectancy—a finding with significant public health implications.
Sun exposure did increase the incidence of melanoma. However, women with higher sun exposure who developed melanoma did not have worse survival outcomes. Sun-associated melanomas tended to be thinner and less aggressive, consistent with prior research linking higher vitamin D levels to less aggressive melanoma at diagnosis. The overall case fatality rate among women who developed melanoma was not significantly different between sun exposure groups.
The authors propose several mechanisms through which sun exposure may reduce mortality. Vitamin D synthesis via UVB radiation is the most discussed candidate, given established associations between low vitamin D and cardiovascular disease, cancer, and metabolic dysfunction. UVA radiation has also been shown to increase nitric oxide bioavailability in the skin, which may lower blood pressure and reduce cardiovascular risk. UVB exposure additionally stimulates cutaneous endorphin release, which may have independent physiological effects.
3) A wandering mind is an unhappy mind
Type of study: Experience sampling study via smartphone application
Sample size: 2,250 adults
Population: Adults aged 18–88 from 83 countries
Key finding: Mind wandering occurred in nearly half of all samples and was a stronger predictor of unhappiness than the activity people were engaged in
This study examined the relationship between mind wandering—thinking about something other than what one is currently doing—and emotional wellbeing in everyday life. Prior research on mind wandering had been conducted almost entirely in laboratory settings with small samples, limiting what could be said about its real-world emotional consequences. The authors addressed this by developing an iPhone application that contacted participants at random moments during waking hours and collected real-time reports of thoughts, feelings, and activities.
The application presented three questions at each contact: a happiness question answered on a continuous scale from 0 (very bad) to 100 (very good), an activity question in which participants selected from 22 options adapted from the day reconstruction method, and a mind wandering question asking whether participants were thinking about something other than what they were currently doing. If yes, they indicated whether the content was pleasant, neutral, or unpleasant. The database contained nearly a quarter of a million samples collected from approximately 5,000 people across 83 countries. The analytical sample for this paper consisted of 2,250 adults with a mean age of 34 years.
Three findings emerged.
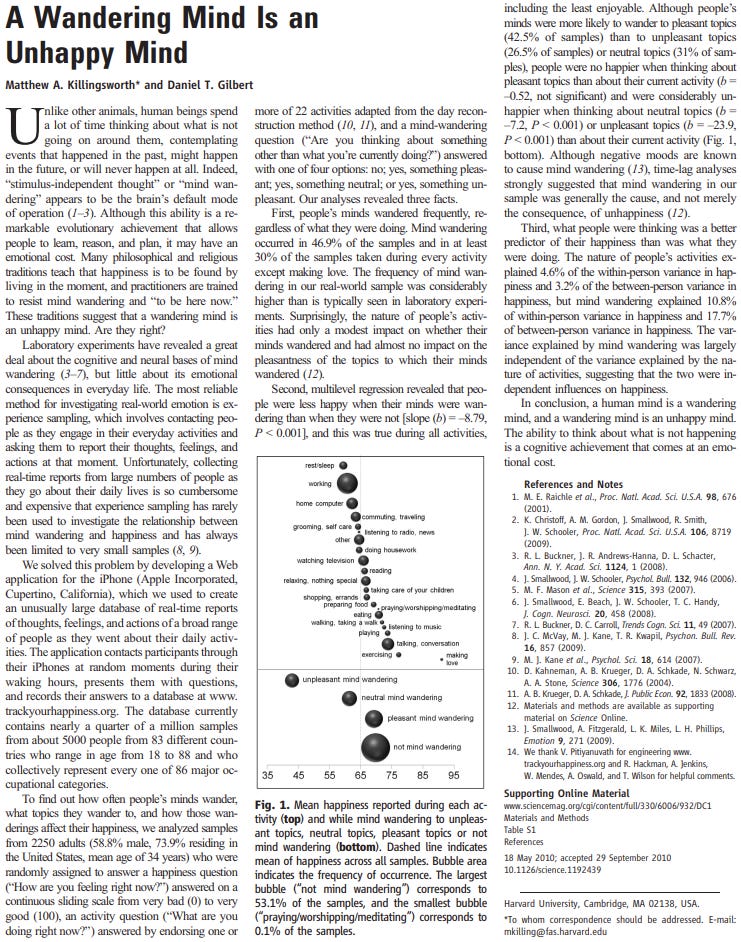
First, mind wandering was extremely common. It occurred in 46.9% of all samples and in at least 30% of samples during every activity measured except one (making love). The frequency was substantially higher than rates typically observed in laboratory experiments, suggesting that controlled settings underestimate how often the mind actually wanders in daily life. The type of activity had only a modest effect on whether the mind wandered and almost no effect on what it wandered to.
Second, people were consistently less happy when their minds were wandering than when they were not, regardless of what they were doing—including during activities they rated as unenjoyable. This held even when mind wandering was to pleasant topics. People thinking about pleasant things were no happier than people focused on their current activity (b = −0.52, not significant). People thinking about neutral topics were meaningfully unhappier (b = −7.2, p < 0.001), and people thinking about unpleasant topics were considerably unhappier still (b = −23.9, p < 0.001). Time-lag analyses—which examined whether unhappiness preceded mind wandering or followed it—suggested that mind wandering was more often the cause of unhappiness than its consequence, though the authors acknowledge this cannot be established with certainty from observational data.
Third, and perhaps most striking, what people were thinking was a better predictor of their happiness than what they were doing. Activity type explained 4.6% of within-person variance in happiness and 3.2% of between-person variance. Mind wandering explained 10.8% of within-person variance and 17.7% of between-person variance. The two were largely independent of each other, suggesting they operate as separate influences on mood rather than one driving the other.
4) The serotonin theory of depression: a systematic umbrella review of the evidence
Type of study: Systematic umbrella review
Sample size: 17 studies included (studies ranged from n = 75 to n = 115,257)
Population: Adults with depressive disorders
Key finding: No consistent evidence that depression is associated with lower serotonin activity or concentrations
The idea that depression is caused by low serotonin—commonly referred to as the “chemical imbalance” theory—has shaped psychiatric practice and public understanding of depression for decades. SSRIs, the most widely prescribed class of antidepressants, were developed on the basis of this theory. This umbrella review set out to systematically evaluate whether the evidence across all major areas of serotonin research actually supports it.
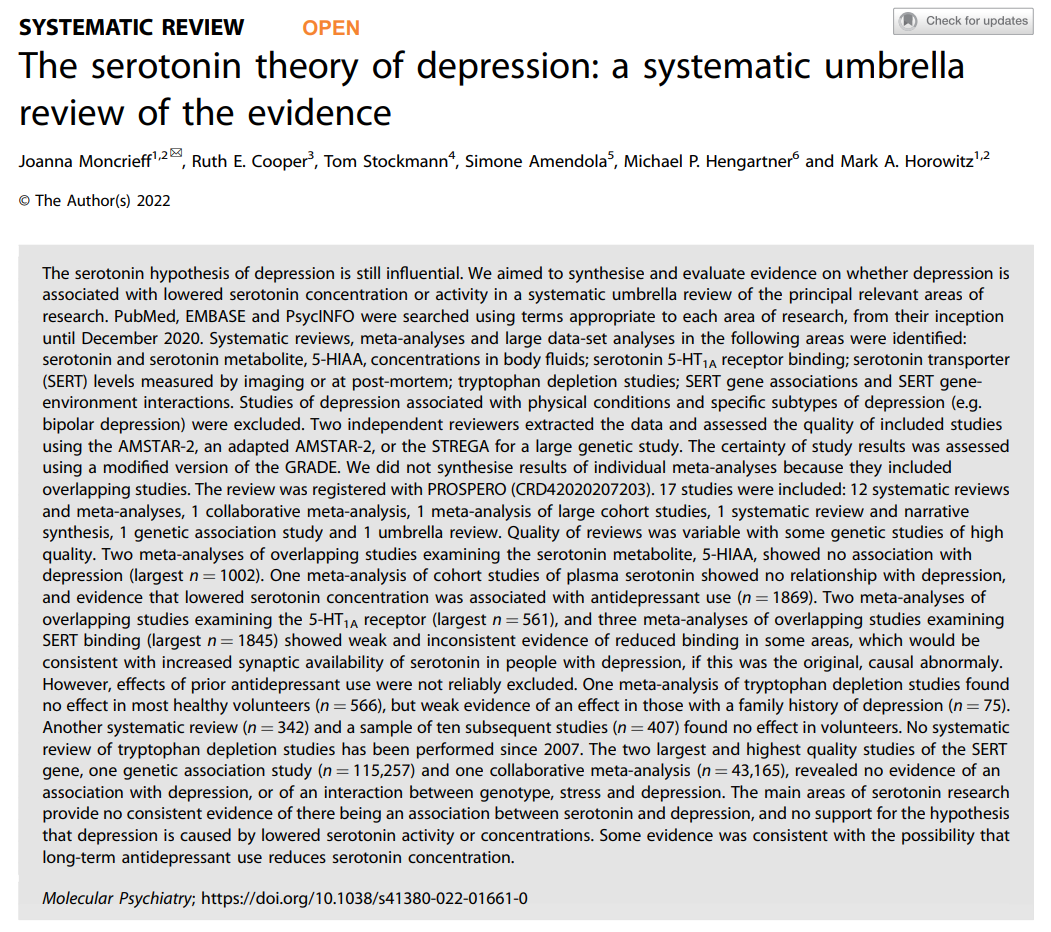
An umbrella review synthesizes existing systematic reviews and meta-analyses rather than individual studies, placing it among the highest levels of evidence synthesis available. The authors searched PubMed, EMBASE, and PsycINFO through December 2020, identifying 17 eligible studies across six research domains: serotonin and its metabolite 5-HIAA in body fluids, serotonin 5-HT1A receptor binding, serotonin transporter (SERT) levels, tryptophan depletion studies, SERT gene associations, and SERT gene-environment interactions. Two independent reviewers extracted data and assessed study quality using established rating tools. The certainty of evidence in each domain was evaluated using a modified GRADE framework.
The findings across all six domains failed to support the serotonin hypothesis.
On serotonin and its metabolite 5-HIAA: Two meta-analyses covering 19 studies found no association between 5-HIAA concentrations in cerebrospinal fluid and depression. A separate meta-analysis of cohort studies found no significant relationship between plasma serotonin and depression. Notably, antidepressant use was independently associated with lower serotonin levels, raising the possibility that some prior findings of reduced serotonin in depressed patients reflected medication effects rather than the underlying condition.
On serotonin receptors: Two meta-analyses of 5-HT1A receptor binding found either no difference between depressed and non-depressed individuals, or lower levels of these inhibitory receptors in depressed patients—which would imply higher, not lower, synaptic serotonin activity. Both analyses were complicated by the fact that most participants had recently used antidepressants or other psychiatric medications.
On the serotonin transporter: Three overlapping meta-analyses found possible reductions in SERT binding in some brain regions, but the results were inconsistent across studies, and most participants had a history of antidepressant use. If the findings do reflect a real effect independent of medication, they would suggest increased rather than decreased synaptic serotonin in depression—the opposite of what the hypothesis predicts.
On tryptophan depletion: Artificially lowering tryptophan—the dietary precursor to serotonin—did not reliably lower mood in healthy volunteers. One small meta-analysis found a minor effect in people with a family history of depression, but the sample was only 75 individuals. Eight of ten recently published depletion studies in healthy volunteers showed no mood effect. The authors note that the most recent comprehensive systematic review of this area was conducted in 2007, leaving a significant gap in the literature.
On genetics: The two largest and highest-quality genetic studies—one involving 115,257 participants and one a collaborative meta-analysis of 43,165—found no association between the serotonin transporter gene (5-HTTLPR) and depression, and no interaction between that gene, stress exposure, and depression risk. Earlier smaller studies had suggested such an interaction, but these were not replicated at scale.
The authors conclude that the evidence does not support the hypothesis that depression is caused by reduced serotonin activity or concentrations. They note that most of the included non-genetic studies were of low methodological quality, did not adequately control for prior antidepressant use, and were based on relatively small samples. The genetic studies were the strongest in the review and provided the clearest negative evidence.
One implication raised in the discussion concerns antidepressant use itself. Evidence from several included studies suggested that long-term antidepressant use may reduce serotonin concentrations—the opposite of their presumed acute mechanism. The authors flag this as an area requiring further investigation, particularly regarding the consequences of prolonged use.
5) Minocycline, a microglial inhibitor, reduces ‘honey trap’ risk in human economic exchange
Type of study: Double-blind, randomized, placebo-controlled trial
Sample size: 98 healthy adult males
Duration: 5 days
Population: Japanese male university students aged 20–30
Key finding: Minocycline eliminated the effect of female physical attractiveness on male trust behavior in an economic exchange
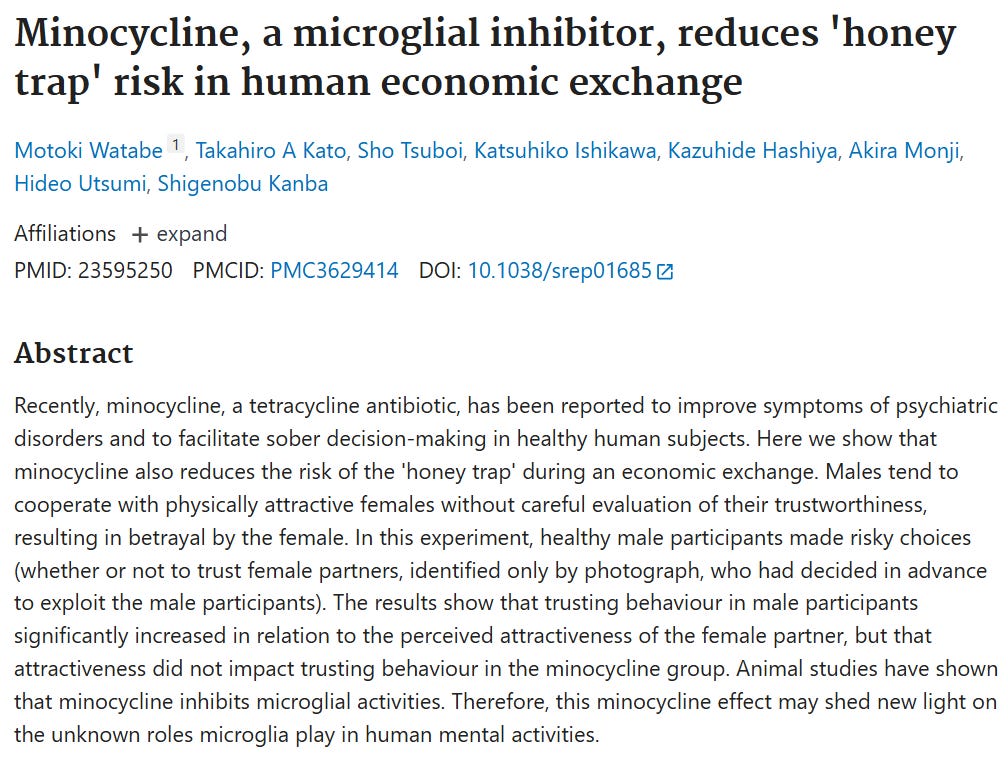
This study examined whether minocycline—a tetracycline antibiotic with known effects on brain immune cells—could reduce a specific bias in male decision-making: the tendency to extend trust to physically attractive females without adequately evaluating their trustworthiness. The researchers called this the “honey trap” effect.
Participants were recruited from Kyushu University and screened by a psychiatrist prior to enrollment. Those with a history of antibiotic side effects, severe organ disease, allergic conditions, or psychiatric disorders were excluded. 101 males were enrolled and 98 completed the full protocol. Participants were randomly assigned in a double-blind manner to receive either 200 mg per day of minocycline or a matched placebo for four days, taken in two daily doses. On day five, approximately three hours after their final dose, participants completed a trust game.
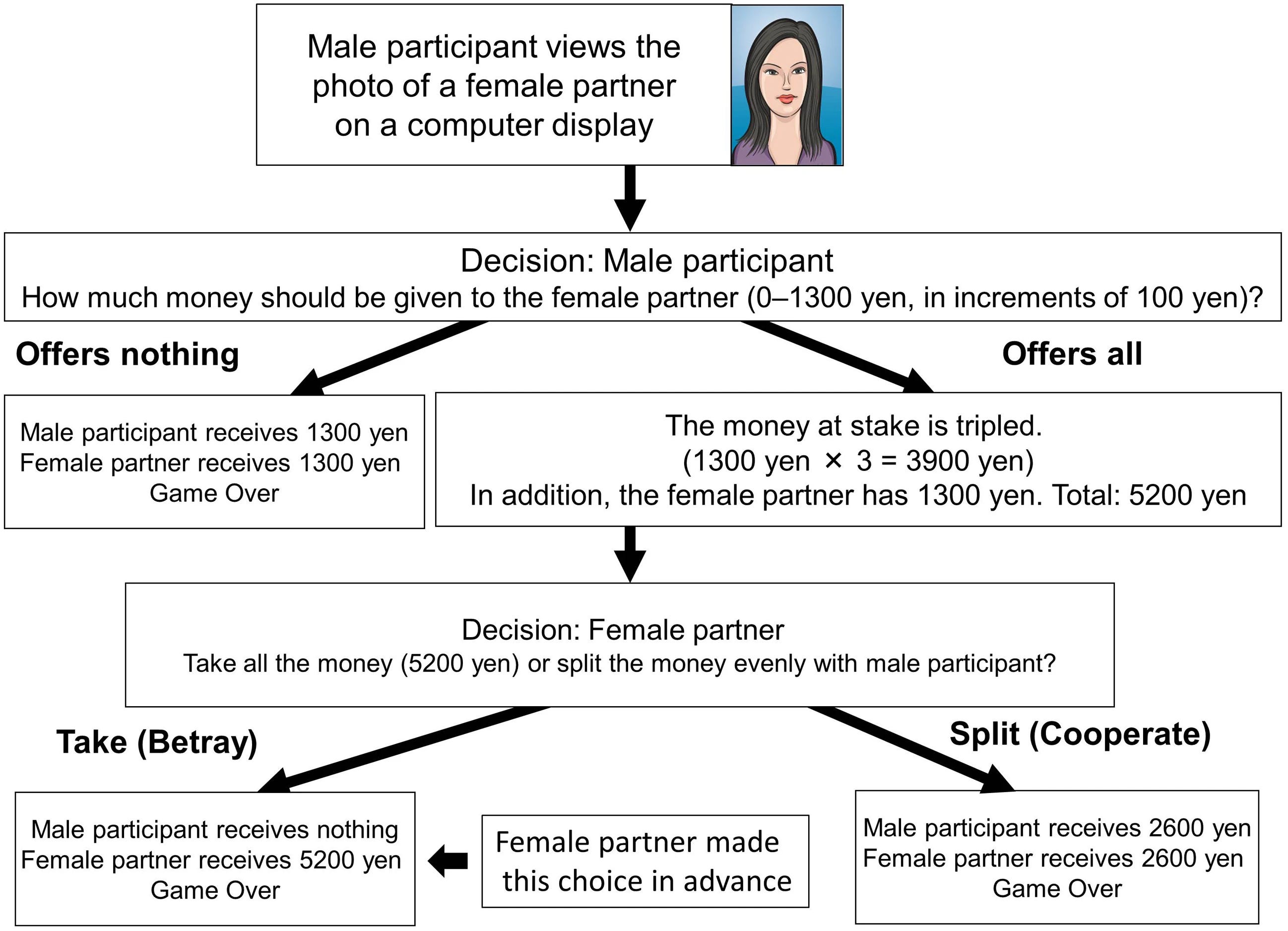
The trust game worked as follows. Each male participant was given 1,300 yen and shown photographs of eight young women, one at a time. For each female partner, the participant decided how much of his 1,300 yen to transfer. Any amount transferred was tripled, after which the female partner would decide whether to split the total equally or keep it all. Crucially, all eight female partners had decided in advance to keep the entire amount—participants were not told this. The amount each male transferred served as the behavioral measure of trust. After each decision, participants rated their female partner on both physical attractiveness and perceived trustworthiness using an 11-point scale.
The results confirmed the honey trap effect in the placebo group. Placebo participants gave significantly more money to partners they rated as more attractive, regardless of perceived trustworthiness (p = 0.0004). The minocycline group showed no such pattern—attractiveness had no significant effect on the amount transferred (p = 0.223). A significant interaction between drug condition and attractiveness was detected (F(1,776) = 7.78, p = 0.005). For highly attractive partners specifically, placebo participants offered significantly more than minocycline participants (p = 0.0004). For less attractive partners, there was no difference between groups (p = 0.590). Anxiety scores did not differ between conditions, suggesting the effect was not mediated by differences in general anxiety state.
The authors propose that the effect operates through minocycline’s inhibition of microglial activity. Microglia are the brain’s resident immune cells, and minocycline is the most commonly used pharmacological tool for suppressing their activity in both animal and human research. Prior clinical work has shown that 200 mg per day of minocycline suppresses microglial activation in regions including the putamen, thalamus, and frontal cortex. The amygdala—a region heavily implicated in evaluating facial trustworthiness—is also reported to be among the brain areas most affected by minocycline. The authors suggest that microglial activity in the amygdala may modulate the cognitive and emotional processes through which attractiveness influences trust judgments, and that minocycline disrupts this pathway.
Alternative mechanisms are acknowledged. Minocycline also affects glutamate and dopamine neurotransmission and has direct effects on neuronal cells, so the observed behavioral change cannot be attributed solely to microglial inhibition. Prior research has also shown that minocycline attenuates the subjective high associated with dextroamphetamine, suggesting a broader capacity to reduce arousal-driven responses—which may partly explain its effect here.
6) Progress on mitochondria and hair follicle development in androgenetic alopecia
Type of study: Narrative review
Scope: Mechanisms linking mitochondrial dysfunction to hair follicle biology, with a survey of existing and emerging treatments for androgenetic alopecia
Key finding: Mitochondrial dysfunction plays a central and underappreciated role in the pathogenesis of androgenetic alopecia, and represents a viable therapeutic target
Androgenetic alopecia (AGA) is the most common form of hair loss, affecting up to 80% of men and 40% of women over a lifetime. The conventional explanation centers on androgens—specifically dihydrotestosterone (DHT), which binds to receptors in hair follicles and causes progressive miniaturization. This review argues that this framing is incomplete, and that mitochondrial dysfunction is a significant and largely overlooked contributor to follicle deterioration.
The authors begin by outlining the basic biology of the hair follicle cycle. Hair follicles pass through three phases: anagen (active growth), catagen (regression), and telogen (rest). The length of the anagen phase determines hair shaft length, and most clinically significant hair loss conditions involve its premature termination. The follicle is maintained by two primary cell populations: hair follicle stem cells (HFSCs), which drive regeneration, and dermal papilla cells (DPCs), which regulate HFSC activation through secreted signaling molecules. Several signaling pathways govern this process, including Wnt/β-catenin, which promotes growth, and TGF-β/BMP, which promotes regression.
Mitochondria intersect with each of these pathways. The review details how mitochondrial reactive oxygen species (ROS) are in fact required for normal Wnt/β-catenin signaling in hair follicles. In mouse models deficient in mitochondrial transcription factor A (TFAM), keratinocytes fail to generate mitochondrial ROS, which disrupts Wnt signaling, reduces β-catenin levels, and causes premature entry into catagen. The same TFAM-deficient models show impaired Notch signaling, with reduced expression of Notch target genes essential for keratinocyte differentiation. Mitochondrial morphology also matters: disruption of the fission protein DRP1 leads to hyperfused mitochondria and inactivates Notch signaling in follicle cells.
The review also covers the role of SIRT1, an NAD-dependent deacetylase that protects HFSCs from inflammation-induced damage via the MAPK-ERK-Mfn2 signaling axis. In AGA specifically, DHT induces mitochondrial dysfunction in DPCs, accelerating their aging and impairing their ability to support HFSC activation. Reduced SIRT1 expression compounds this by triggering a TNF-α-mediated inflammatory stress response in HFSCs. The authors present this as a plausible mechanistic link between androgen exposure and the cellular energy deficits observed in miniaturizing follicles.
Several mitochondrial proteins are discussed in relation to follicle health. CRIF1, a mitochondrial ribosomal protein, is required for oxidative phosphorylation and β-catenin signaling—its absence in mouse models produces abnormal hair morphology and delayed hair cycle progression. Apoptosis-inducing factor (AIF), located in the inner mitochondrial membrane, facilitates the anagen-to-catagen transition through caspase-independent apoptosis. Impaired AIF activity produces irregular follicle cycling. MPZL3, a nuclear-encoded mitochondrial protein, regulates ROS production and lipid metabolism in sebaceous glands, and its disruption causes premature anagen entry and seborrheic dermatitis-like inflammation. Krtap11-1, a mitochondrially located protein, modulates Wnt and BMP signaling and peaks in expression during catagen and telogen—its dysfunction leads to weak hair shafts and increased oxidative stress.
The thyroid axis is also discussed. Thyroid hormones stimulate mitochondrial biogenesis and prolong the anagen phase by promoting keratinocyte proliferation and keratin expression. Expression of the mitochondrial protein MTCO1 is upregulated in scalp hair follicles under the influence of the hypothalamus-pituitary-thyroid axis, supporting follicle growth. Mitochondrial dysfunction arising from hormonal imbalance can impair ATP production and compromise the energy supply available for follicle maintenance.
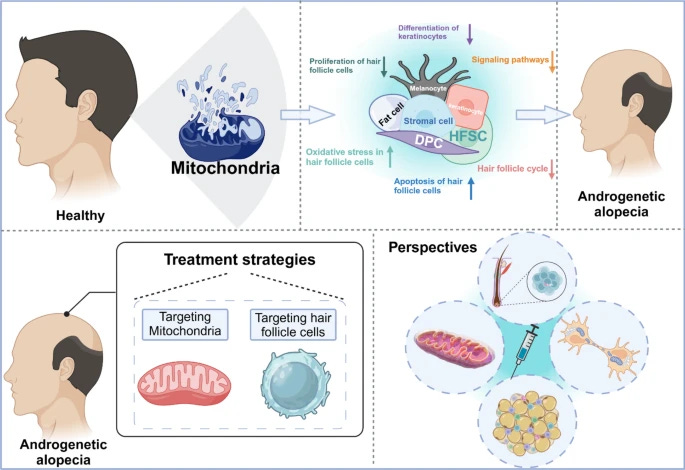
On the treatment side, the review surveys both established and emerging approaches. Minoxidil is discussed in the context of mitochondrial function—it may act partly by elevating intracellular calcium levels and increasing ATP synthase activity, though this mechanism remains incompletely characterized. Low-level laser therapy is proposed to work by stimulating mitochondrial photon absorption, increasing ATP production and nitric oxide release, and improving local blood circulation. Melatonin is highlighted for its antioxidant and DNA repair properties, reducing ROS and supporting SIRT1-mediated protection against oxidative damage in follicle cells. N-acetylcysteine (NAC) is noted as a mitochondria-targeted antioxidant that improved hair growth in men with early-onset AGA in at least one trial. Cyanidin-3-O-arabinoside (C3A) is identified as a compound that reduces DHT-induced slowing of hair growth by preventing mitochondrial calcium accumulation.
The review also covers novel drug delivery approaches, including microneedle patches integrated with cerium nanozymes capable of delivering antioxidants approximately 300 microns into the skin, and mitochondria-targeted antioxidants such as MitoQ and SkQ1, which are designed to accumulate preferentially within mitochondria. Mitochondrial transfer—transplanting functional mitochondria from healthy donor cells into damaged cells—is discussed as an experimental direction, with early evidence from non-hair contexts showing restoration of bioenergetic capacity and reduced oxidative stress.
7) The tenacious brain: how the anterior mid-cingulate contributes to achieving goals
Type of study: Narrative review
Scope: Neuroanatomy, functional neuroimaging, lesion studies, and stimulation studies examining the role of the anterior mid-cingulate cortex in tenacity, motivation, and goal-directed behavior
Key finding: The anterior mid-cingulate cortex functions as a central hub for integrating cost-benefit computations that underlie persistence in the face of challenge, and its structure and function predict outcomes across health, aging, academic achievement, and neuropsychiatric illness
This review argues that a specific brain region—the anterior mid-cingulate cortex (aMCC)—is the neurological seat of tenacity. The authors define tenacity as a bias in effort computations by which the costs of effort are devalued and the value of long-term rewards is emphasized, driving persistence in the face of difficulty. The paper synthesizes evidence from neuroanatomy, functional imaging, lesion studies, and direct brain stimulation to support this claim.
The aMCC sits at the intersection of at least five partially overlapping intrinsic brain networks, including systems involved in executive function, autonomic regulation, interoception, motor control, and attention. Structural connectivity analyses show the aMCC has strong connections with the dorsal prefrontal cortex, anterior and posterior insula, thalamus, amygdala, hypothalamus, premotor cortex, and periaqueductal gray. Network analyses consistently identify it as one of the most broadly connected regions in the brain—a structural and functional hub in the same class as other high-traffic regions known to coordinate activity across otherwise segregated systems.
Functionally, the aMCC is among the most consistently activated regions in the fMRI literature. A meta-analysis of over 5,600 studies found it to be one of the most frequently reported activation sites across diverse task domains including pain, negative affect, reward processing, memory, cognitive control, motor planning, social cognition, and autonomic reactivity. The authors argue this cross-domain engagement reflects a single underlying function: computing the expected energetic cost and reward value of potential actions, and allocating physiological and attentional resources accordingly.
The case for the aMCC’s role in tenacity specifically rests on several converging lines of evidence.
On lesion studies: damage to the aMCC or its connections consistently produces motivational impairment. In a case study of a patient with an aMCC lesion, the individual could perform cognitively demanding tasks at a relatively normal level but reported no subjective sense of effort and showed no increase in skin conductance as task difficulty increased—suggesting the aMCC is specifically required for registering the cost of effort rather than performing the task itself. In animal models, inactivation of the homologous region reduces willingness to expend mental effort and decreases the energy expenditure animals are prepared to commit to obtain a proportional reward.
On neuroimaging: several studies have linked aMCC structure and function directly to measures of tenacity. Spontaneous aMCC activity predicts grit scores. Greater functional connectivity between the aMCC and the striatum predicts both grit and growth mindset. Stronger structural and functional connectivity between the aMCC and the supplementary motor area predicts lower levels of apathy. aMCC activity during effort-based decision tasks predicts willingness to choose more demanding options and predicts trait-level persistence. Greater gray matter volume in the aMCC also predicts persistence as measured by personality inventory.
On stimulation: direct electrical stimulation of the aMCC in human patients produces what has been described as an increase in the will to persevere. In a well-controlled study across 329 patients and 1,789 cingulate stimulation sites, stimulation of the aMCC reliably elicited goal-oriented behaviors and a subjective sense of preparation for challenge. One patient described the feeling as: being headed toward a storm and having to figure out how to get through it. Transcranial stimulation targeting the aMCC has also been shown to reduce self-reported appetite in women with obesity, suggesting that augmenting aMCC activity can modulate self-regulatory behavior.
The review draws out several applied implications. In depression, aMCC volume reduction predicts severity of apathetic symptoms, and depressed individuals show reduced aMCC activation during planning tasks and impaired error-related aMCC responses—consistent with the view that motivational deficits in depression reflect disrupted aMCC function rather than hedonic processing alone. In neurodegenerative disease, apathy across Alzheimer’s disease, frontotemporal dementia, and Parkinson’s disease is linked to abnormal aMCC metabolism and connectivity in each case. In aging, a subgroup of older adults known as superagers—whose episodic memory performance matches that of much younger adults—show aMCC cortical thickness and network connectivity equivalent to young controls, and this preserved structure predicts memory performance. The authors propose that superagers may persist longer on cognitively demanding tasks due to superior aMCC function, effectively training the region through continued challenge.
On exercise and obesity, aMCC metabolism correlates with exercise intensity and is more strongly coupled in individuals with greater exercise capacity. Regular aerobic exercise has been associated with increased gray matter volume in frontal regions including the aMCC, raising the possibility that the region can be structurally strengthened through sustained physical training. Individuals who have successfully maintained weight loss after obesity show substantially enhanced aMCC activation in response to food cues compared to controls, suggesting that aMCC-mediated cognitive control is a distinguishing feature of sustained behavioral change.
8) Refined carbohydrate consumption and facial attractiveness
Type of study: Observational cross-sectional study
Sample size: 99 subjects (50 women, 49 men), 150 attractiveness raters, 222 age-estimation raters
Population: Caucasian university students aged 18–26
Key finding: Higher between-meal glycaemic load was associated with increased facial attractiveness ratings by opposite-sex raters in both men and women
This study examined whether refined carbohydrate consumption is associated with facial attractiveness. The rationale was physiological: chronic consumption of refined carbohydrates generates hyperglycaemia and hyperinsulinaemia, both of which interfere with sex hormones and growth factors that influence facial morphology and skin aging. If these downstream effects are visible in the face, they may be detectable by opposite-sex raters.
Subjects were recruited from the University of Montpellier. All reported European ancestry across all four grandparents. Standardized frontal facial photographs were taken under controlled conditions—neutral expression, no glasses or earrings, uniform gray background, and consistent camera settings. Physical characteristics including height, weight, smoking status, scholarship level, and contraceptive pill use in women were recorded as control variables.
Dietary assessment focused on three meals considered to carry higher glycaemic risk: breakfast, afternoon snack, and between-meal snack. These meals tend to be higher in refined carbohydrates and lower in fat, protein, and fiber—a composition that produces larger glycaemic and insulinaemic responses. For each food and drink item consumed at these meals, glycaemic load (GL) was calculated using established international tables. Glycaemic load accounts for both the glycaemic index of a food and the quantity consumed, making it a more precise proxy for glycaemic and insulinaemic response than glycaemic index alone. Separate GL scores were computed for breakfast (GL1), afternoon snack (GL2), and between-meal snack (GL3).

Two separate panels of raters were recruited from public places in Montpellier. One panel estimated the apparent age of subjects from their photographs. A second panel assessed attractiveness by choosing the more attractive face from pairs of same-sex photographs, with all pairs rated by opposite-sex raters. Raters with poor reliability—based on repeated trials built into the procedure—were excluded. The final attractiveness analysis included 150 raters evaluating 99 subjects.
A facial femininity/masculinity index was computed using geometric morphometric analysis of 142 facial landmarks, which was then reduced to a single discriminant score separating male and female facial morphology. This index served as a control variable in the attractiveness models.
The primary finding was that GL3—the between-meal glycaemic load—significantly predicted attractiveness in both sexes. Men with higher GL3 were preferred by female raters (β = 0.564, p = 0.001), and women with higher GL3 were preferred by male raters (β = 0.468, p = 0.007). GL1 and GL2 showed no significant effect in either sex. The direction of this result—higher refined carbohydrate consumption associated with greater attractiveness—was the opposite of what the authors predicted based on known physiological effects, particularly for women, where hyperinsulinaemia-driven androgen elevation would be expected to increase facial masculinity and reduce attractiveness.
Structural equation modeling was used to explore whether GL3 acted on attractiveness indirectly through the control variables. For men, higher GL3 was associated with an increase in apparent age relative to chronological age, and appearing older within the 18–26 range was independently associated with higher attractiveness among female raters, which is consistent with prior evidence that women prefer men who display cues of resource acquisition and social status. For women, higher GL3 showed a marginally significant association with increased facial femininity (p = 0.056), which the authors suggest may reflect hyperinsulinaemia-driven sex hormone changes, though they acknowledge this runs counter to expectation and requires further investigation.
The authors offer an evolutionary interpretation for the unexpected direction of the effect. In pre-industrial environments, foods that generate hyperglycaemia (e.g. ripe fruit, honey) were scarce and seasonally limited. The ability to access them may have served as a reliable signal of foraging success or resource quality, making facial cues of such consumption attractive to potential mates. In the modern dietary environment, where refined carbohydrates are ubiquitous, this preference may represent a maladaptation—a response calibrated for scarcity that no longer tracks actual resource quality.
9) Meal timing trajectories in older adults and their associations with morbidity, genetic profiles, and mortality
Type of study: Longitudinal cohort study
Sample size: 2,945 community-dwelling older adults
Duration: Up to 34 years of follow-up (1983–2017)
Population: Adults aged 42–94 at enrollment
Key finding: Later breakfast timing was associated with increased physical and psychological illness, evening chronotype genetics, and higher all-cause mortality risk
This study examined how meal timing changes across older adulthood and what those changes mean for health and survival. Most prior research in chrononutrition—the study of when food is eaten and its effect on health—has focused on younger adults or cross-sectional snapshots. This paper used nearly four decades of longitudinal data to track meal timing trajectories in the same individuals over time.
Participants were drawn from the University of Manchester Longitudinal Study of Cognition in Normal Healthy Old Age (UMLCHA), which enrolled 6,375 adults starting in 1983. Of these, 2,945 had complete meal timing data at baseline and at least one follow-up assessment. Participants completed a Personal Details Questionnaire up to five times across the study period, reporting the times they ate breakfast, lunch, and dinner, as well as when they went to bed and woke up. From these responses, the researchers derived several variables: the interval between waking and breakfast, the interval between dinner and bed, the daily eating window, and the eating midpoint. Mortality data were obtained from the NHS Digital death registry through August 2017.
Health status was assessed using the Cornell Medical Index, a validated instrument covering 19 areas of physical and psychological symptomatology, administered on four occasions. A multimorbidity index was calculated by summing the number of conditions reported at each assessment. A subset of 1,226 participants also provided blood samples for genetic analysis, from which polygenic scores for evening chronotype and obesity were derived.
On meal timing trajectories, the data showed that with each additional decade of age, breakfast shifted later by approximately 8 minutes in the unadjusted model and 3 minutes after full adjustment. Dinner also shifted later with age, and the eating midpoint moved later while the total daily eating window shortened. Lunch timing remained stable across the follow-up period, likely because of limited variability in midday schedules across the sample. Across the full age range of participants, the cumulative shift in breakfast timing amounted to approximately 45 minutes.
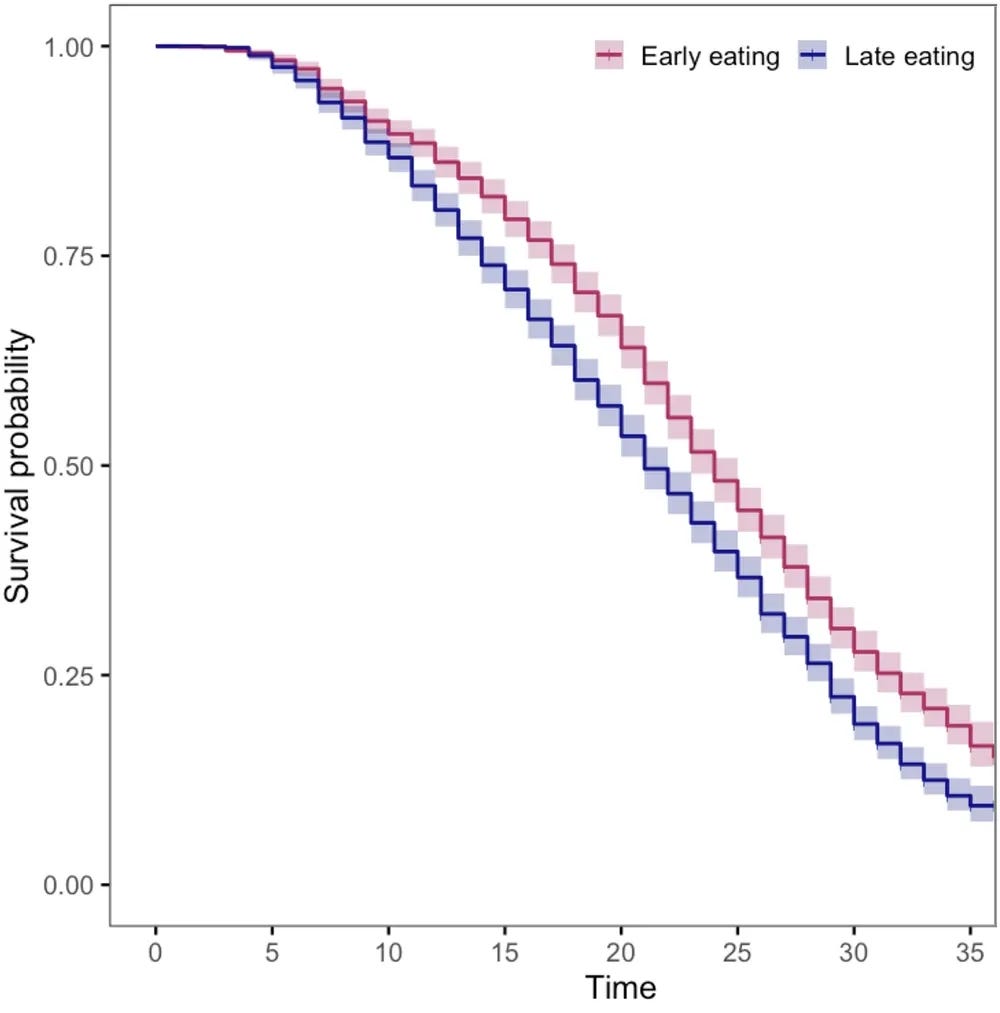
Latent class analysis identified two distinct subgroups: an early eating group of 1,391 participants who maintained consistently earlier meal times with age, and a late eating group of 1,554 participants whose meal times shifted progressively later. These groups showed meaningful differences in survival.
On morbidity, later breakfast timing was associated with depression, fatigue, hypochondria, and multimorbidity. Anxiety was associated with a shorter eating window. Oral health problems were associated with earlier dinner and a shorter eating window. These associations held after adjusting for lifestyle factors including sleep duration, smoking, alcohol, employment status, and marital status.
On genetics, each standard deviation increase in the polygenic score for evening chronotype was associated with breakfast being later by 7.2 minutes, lunch by 3.1 minutes, and dinner by 3.9 minutes. The obesity polygenic score was not associated with meal timing after adjustment, suggesting that genetic predisposition toward evening behavior—rather than body weight genetics—is the stronger driver of late eating patterns in this population.
On mortality, 2,361 deaths were recorded over 63,388 participant-years of follow-up. Each additional hour of later breakfast timing was associated with an 11% increase in mortality risk in the unadjusted model (HR 1.11, 95% CI 1.03–1.18) and an 8% increase after full adjustment (HR 1.08, 95% CI 1.00–1.17). The 10-year survival rate was 89.5% in the early eating group compared to 86.7% in the late eating group. No significant mortality associations were found for lunch timing, dinner timing, eating window length, or proximity of dinner to bedtime.
The authors are careful about directionality. Because the study is observational, the more plausible interpretation is that illness drives later meal timing rather than the reverse—depression, fatigue, and poor oral health make it harder to eat at regular times, and those same conditions predict higher mortality. Later breakfast may therefore function primarily as a marker of underlying health decline rather than a direct cause of increased mortality risk. The authors suggest this still has clinical value, as shifts in breakfast timing could serve as an early, easily detectable indicator of health deterioration in older adults.
10) Emotional suppression and mortality risk over a 12-year follow-up
Type of study: Prospective cohort study
Sample size: 729 adults
Duration: 12 years (1996–2008)
Population: Nationally representative sample of non-institutionalized US adults aged 18 and over
Key finding: Higher emotion suppression was associated with a 35% increase in all-cause mortality risk and a 70% increase in cancer mortality risk
This study examined whether the tendency to suppress emotional expression is associated with a higher risk of death over a 12-year follow-up period. Prior research had suggested a link between emotion suppression and chronic disease, but evidence on mortality specifically was limited, methodologically contested, or drawn from non-representative samples. This paper used a nationally representative US dataset linked to official death records to provide a more rigorous test of the association.
Data came from the 1996 General Social Survey (GSS), an annual nationally representative study of US adults conducted by the National Opinion Research Center. In 1996, a six-item emotion suppression scale was administered to 737 respondents. The scale asked participants to rate their agreement with statements such as “I keep my emotions to myself,” “When I’m angry I let people know,” and “I try to be pleasant so that others won’t get upset.” Responses were made on a five-point Likert scale, with higher scores indicating greater suppression. The GSS data were subsequently linked to the US National Death Index, which records cause of death with a verified accuracy rate of 99.8%. Of the 729 participants with complete data, 111 died during the follow-up period—37 from cardiovascular disease and 34 from cancer.
Mortality associations were assessed using Cox proportional hazards models adjusted for age, sex, minority race and ethnicity, education, and self-rated health. Suppression scores were scaled by the interquartile range, so reported hazard ratios reflect the difference between someone at the 75th percentile of suppression versus someone at the 25th percentile—a practically meaningful comparison rather than a theoretical one-unit shift.
The primary finding was that higher emotion suppression was associated with a 35% increase in all-cause mortality risk (HR 1.35, 95% CI 1.00–1.82, p = 0.049). For cancer mortality specifically, the association was larger—a 70% increase in risk (HR 1.70, 95% CI 1.01–2.88, p = 0.049). The association with cardiovascular disease mortality was in the same direction but did not reach statistical significance (HR 1.47, 95% CI 0.87–2.47, p = 0.148). When deaths in the first year were removed to reduce the possibility that pre-existing illness drove the results, the effects strengthened: all-cause mortality risk increased to 42% (HR 1.42, p = 0.028) and cancer mortality risk to 108% (HR 2.08, p = 0.013).
Exploratory analyses of individual scale items found that higher anger suppression, specifically disagreeing more strongly with “When I’m angry I let people know,” was associated with elevated risk across all three mortality outcomes. Disagreeing more with “I’m not afraid to let people know my feelings” was significantly associated with cancer mortality. Both items involve emotional expression toward others, which the authors interpret as consistent with research on the health-protective effects of social support and interpersonal emotional disclosure.
The authors propose two broad mechanisms through which suppression may influence mortality. At a behavioral level, suppression may lead to unhealthy coping behaviors (e.g. overeating, social withdrawal) as substitutes for emotional expression. At a physiological level, suppression has been associated with greater autonomic reactivity to stress and with elevated levels of catecholamines and glucocorticoids, suggesting that habitual suppression may dysregulate neuroendocrine systems in ways that contribute to disease progression over time.
If any of these papers changed how you think about something, that is exactly the point. There is considerable value in developing an independent relationship with scientific literature. Reading original research provides a more complete and accurate picture than someone else’s interpretation. The papers are out there, and most are freely accessible. The only requirement is your willingness to look.
Thank you for reading.