
Health Modalities More Effective Than SSRIs at Treating Depression
Seven evidence-backed interventions for depression

Antidepressants are among the most prescribed drugs in the world.
In the United States alone, more than 1 in 10 adults takes them—a figure that has risen nearly 60% over the past decade. [1]
The rationale behind the most common class—selective serotonin reuptake inhibitors, or SSRIs—follows an outdated and inaccurate framework that is used to sell ineffective and side-effect-ridden pharmaceutical drugs to 29 million Americans.
That framework is the chemical imbalance theory.
This is the idea that depression is caused by a deficiency of serotonin in the brain. SSRIs are said to “correct” this “deficiency” by blocking serotonin reuptake, leaving more of it available at the synapse.
What SSRIs do in practice is reduce the intensity of negative emotions while simultaneously limiting the capacity for positive ones. This leaves many individuals in an anhedonic and dissociated state where they can’t quite feel anything at all.
In 2022, a systematic umbrella review published in Molecular Psychiatry evaluated every principal area of serotonin research:
Metabolite studies
Receptor binding
Transporter levels
Tryptophan depletion
Gene associations
Across all of them, the review found no consistent evidence that depression is associated with lowered serotonin activity. [2] The chemical imbalance theory, on which decades of SSRI prescribing has been based, didn’t hold up to this review.
Furthermore, a growing body of research shows that several accessible, low-cost health modalities are at least as effective as SSRIs for mild-to-moderate depression, and in many cases more so.
This article outlines the evidence for each of them.
I am not a doctor. None of this is medical advice. It reflects my personal experience and research. Do your own due diligence and consult with your doctor before trying anything discussed here.
1) Exercise
Exercise has the strongest evidence of any intervention in this article.
A 2024 network meta-analysis published in the BMJ—pooling 218 randomized controlled trials involving over 14,000 participants—found that exercise was as effective as antidepressants and psychotherapy for mild-to-moderate depression. [3]
Resistance training is particularly supported by the data.
A 2025 meta-analysis pooling randomized controlled trials in adults with clinically diagnosed depression found a large antidepressant effect (pooled SMD = −0.94), comparable in magnitude to what SSRIs produce in the most favorable trials, and without any side effects. Effects were observed in both primary depressive disorder and depression occurring alongside other conditions. [4]
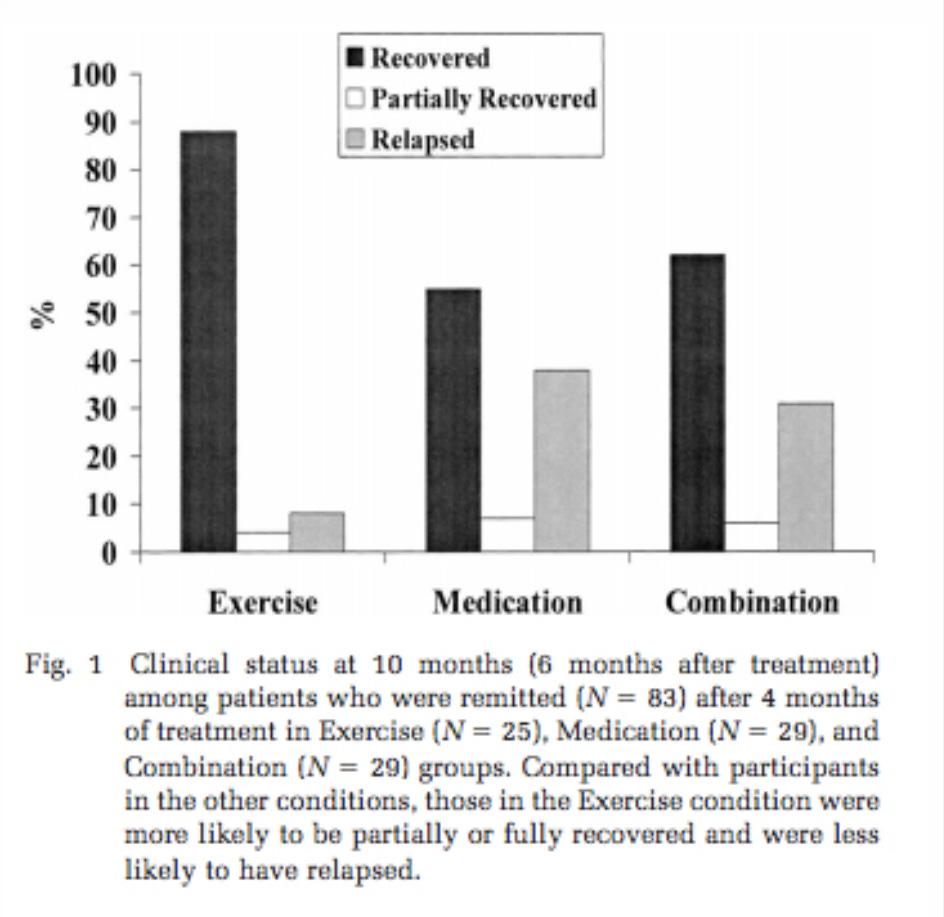
The strongest effects of all came from combining aerobic and resistance training.
A 2025 meta-analysis of 27 randomized controlled trials involving 2,342 patients found a pooled SMD of −1.39, larger than either modality alone. Effects were most pronounced in middle-aged and elderly patients with moderate depression. The optimal prescription across the included trials was 3 to 4 sessions per week, sustained over 9 to 24 weeks, with more than 180 minutes of total weekly activity. [5]
Mechanisms include:
HPA (hypothalamic-pituitary-adrenal) axis regulation: Exercise reduces cortisol dysregulation, which is a known cause of depression
Increased production of BDNF (brain-derived neurotrophic factor): Supports neuroplasticity and the growth of new neurons
Reduced systemic inflammation: Chronic inflammation is consistently elevated in depressed populations and directly impairs mood regulation
Improved sleep quality: Disrupted sleep both causes and worsens depression; exercise is one of the most effective interventions for it
2) Light Therapy
Light therapy is inexpensive, requires no prescription, and in non-seasonal depression has demonstrated remission rates comparable to antidepressants.
A 2024 systematic review and meta-analysis of 11 randomized controlled trials—involving data on more than 850 participants—found that bright light therapy produced a 41% remission rate in non-seasonal depression, significantly higher than comparison conditions including antidepressants alone and placebo controls. [6]
A separate 2024 meta-analysis of 15 randomized controlled trials involving 883 patients confirmed a significant positive effect on major depressive disorder. Effects appeared strongest with longer daily exposures of 60 minutes or more. [7]
The mechanism is well established.
Bright light stimulates melanopsin-containing retinal ganglion cells, which regulate the suprachiasmatic nucleus—the brain’s primary circadian pacemaker. This in turn affects the synthesis of neurotransmitters and melatonin regulation. Many depressed patients exhibit disrupted circadian rhythms, irregular sleep-wake patterns, and circadian mood swings.
3) Saffron
Saffron is the most compelling herbal intervention in this article, and the most directly comparable to SSRIs.
A 2025 meta-analysis published in Nutrition Reviews—pooling 8 randomized controlled trials in adults with depression—found no statistically significant difference between saffron and SSRIs in reducing depressive symptoms (SMD = 0.10; 95% CI: −0.09 to 0.29). The analysis also examined anxiety outcomes across 4 trials, finding no significant difference there either (SMD = 0.04; 95% CI: −0.22 to 0.29).
In terms of safety, saffron performed better than SSRIs. Participants taking it had fewer adverse events than those on SSRIs, with lower rates of nausea, vertigo, and sexual dysfunction. The authors concluded that saffron represents a viable alternative to SSRIs for mild-to-moderate depression, with a favorable tolerability profile. [8]

Crocin, crocetin, and safranal—the active compounds in saffron—act through several distinct mechanisms:
Its anti-inflammatory activity reduces pro-inflammatory cytokines, which are consistently elevated in depressed populations
Crocin inhibits the reuptake of dopamine and norepinephrine, while safranal inhibits serotonin reuptake
It acts as a GABA-A agonist, promoting inhibitory neurotransmission and reducing anxiety alongside depressive symptoms
Its antioxidant activity reduces oxidative stress, which impairs neuronal function and is associated with depression
Saffron exhibits NMDA receptor antagonism, reducing excitotoxic activity that is implicated in neuronal damage and depression
It upregulates BDNF, supporting neuroplasticity and the growth of new neurons
4) Vitamin D3
Vitamin D3 is a fat-soluble vitamin and secosteroid hormone that regulates hundreds of physiological processes, including several that are directly implicated in depression.
Low serum vitamin D is one of the most prevalent nutritional deficiencies in the developed world, and its association with depression is well established across both observational and interventional research.

A dose-response meta-analysis published in Psychological Medicine—pooling 31 randomized controlled trials involving 24,189 participants—found that each additional 1,000 IU per day of vitamin D3 produced a statistically significant reduction in depressive symptoms (SMD = −0.32; 95% CI: −0.43 to −0.22).
Effects were more pronounced in individuals who already had depressive symptoms at baseline (SMD = −0.57), and strongest at higher doses—the greatest reduction was observed at 8,000 IU per day. Interestingly, shorter supplementation periods of eight weeks or less produced stronger effects than longer regimens. [9]
Vitamin D receptors (VDRs) are expressed throughout the central nervous system, including in the prefrontal cortex, hippocampus, and hypothalamus—regions consistently implicated in mood regulation and depressive pathology.
Vitamin D3 regulates the transcription of tryptophan hydroxylase, the rate-limiting enzyme in serotonin synthesis, and tyrosine hydroxylase, which governs dopamine synthesis. It also modulates glucocorticoid receptor sensitivity and suppresses HPA axis hyperactivity. Additionally, vitamin D3 exerts anti-inflammatory effects through downregulation of pro-inflammatory cytokines including TNF-α and IL-6, both of which are consistently elevated in depressed populations and have been shown to impair monoamine synthesis and neuroplasticity.
5) Magnesium
Magnesium is the fourth most abundant mineral in the body.

A 2012 analysis identified 3,751 magnesium-dependent processes in human physiology. It is also deficient in an estimated half of the US population, which has direct relevance to the prevalence of depression.
A 2023 systematic review and meta-analysis published in Frontiers in Psychiatry—pooling 7 randomized controlled trials in adults with clinically diagnosed depressive disorder—found that magnesium supplementation produced a significant reduction in depression scores (SMD = −0.919; 95% CI: −1.443 to −0.396).
This is a large effect size, comparable in magnitude to the resistance training data covered earlier in this article, and substantially larger than the mean effect reported across SSRI trials. [10]
The mechanisms are well characterized.
Magnesium acts as a natural antagonist at NMDA receptors, blocking excessive glutamatergic activity that is implicated in neuronal excitotoxicity and depression. It regulates the HPA axis, reducing cortisol output under conditions of chronic stress. It also modulates GABA receptor activity, promoting inhibitory neurotransmission. Low intracellular magnesium concentrations have been found consistently in depressed patients, and animal models of magnesium depletion reliably produce depressive and anxiety-like behavior.
Not all magnesium supplements are equal in terms of bioavailability. Magnesium oxide (the most common form in cheap supplements) is poorly absorbed. The forms with the best absorption and tolerability are magnesium glycinate and magnesium taurate. The dose range used across the clinical trials is 248 to 500 mg of elemental magnesium per day.
6) Zinc
Serum zinc is consistently lower in depressed individuals than in healthy controls.
A meta-analysis of 17 observational studies measuring peripheral blood zinc concentrations in 1,643 depressed and 804 control subjects found that zinc concentrations were approximately 1.85 µmol/L lower in depressed individuals than in controls. The severity of depression correlated with the degree of zinc deficiency. [11]
The interventional evidence supports supplementation.
A dose-response meta-analysis of observational studies and randomized controlled trials—published in General Hospital Psychiatry—found that zinc supplementation significantly lowered depressive symptom scores (WMD = −4.15 points; 95% CI: −6.56 to −1.75), and that the highest level of dietary zinc intake was associated with a 28% reduced risk of depression. Notably, significant improvement in depression scores was observed specifically when zinc was used as a monotherapy rather than in combination with antidepressant medications. [12]
The mechanisms are consistent with what is known about zinc’s role in neurological function. Zinc modulates NMDA receptor activity and glutamate homeostasis, regulates HPA axis function, and is involved in BDNF signaling—the same pathways implicated in the antidepressant effects of exercise and magnesium. Zinc deficiency leads to HPA axis hyperactivation and elevated corticosterone, which directly impairs neuroplasticity and mood regulation.
7) Sleep
Depression and sleep disruption both involve HPA axis dysregulation, circadian rhythm disruption, and inflammatory signaling. Understanding this relationship reframes sleep not as a passive symptom of depression but as an active driver of it.
The mechanism runs primarily through the HPA axis. Poor sleep quality and reduced sleep duration increase cortisol secretion throughout the day, sustain HPA axis hyperactivation, and reduce glucocorticoid receptor sensitivity—the same pathway implicated in the pathophysiology of depression. Simultaneously, circadian rhythm disruption impairs the synthesis of melatonin, reduces BDNF expression, and elevates pro-inflammatory cytokines including IL-6 and TNF-α. Insomnia is now recognized as an independent risk factor for the development of depression, not merely a secondary symptom of it. [13]
Several simple, evidence-informed practices address these mechanisms directly.
Morning sunlight exposure is one of the most effective tools for circadian entrainment. Light exposure in the first hour after waking suppresses residual melatonin, triggers a cortisol awakening response that is properly timed, and sets the circadian clock for the following night’s sleep. [14] Even on overcast days, outdoor light exposure produces a significantly stronger circadian signal than indoor lighting. Ten to thirty minutes of outdoor exposure each morning is sufficient for most people.
Artificial light at night, particularly blue-spectrum light from screens and overhead lighting, suppresses melatonin secretion and delays circadian phase. [15] Blue light blocking glasses, or switching devices to warm-toned night mode settings after sunset, attenuate this effect. Dimming overhead lighting in the two hours before bed produces a similar result.
Reading before bed, physical books rather than screens, reduces pre-sleep cognitive arousal and has been shown to reduce time to sleep onset. The mechanism is partly attentional displacement and partly the absence of blue light stimulation.
Several supplements have reasonable evidence for improving sleep quality without the dependency risks associated with pharmaceutical sleep aids:
Magnesium glycinate (200–400 mg): Reduces HPA axis activation, promotes GABA-A activity, and shortens sleep onset latency [10]
L-theanine (200–400 mg): An amino acid found in green tea that promotes alpha wave activity and reduces pre-sleep anxiety without sedation [16]
Glycine (3 g): Reduces core body temperature, which is a physiological prerequisite for sleep onset, and has been shown in RCTs to improve subjective sleep quality and reduce daytime fatigue [17]
Apigenin (50 mg): A flavonoid found in chamomile that binds GABA-A receptors and produces mild sedative effects without grogginess the next day [18]
Conclusion
Every intervention in this article targets the underlying cause of depression.
The evidence behind them (e.g. randomized controlled trials, systematic reviews, meta-analyses) is the same category of evidence used to evaluate pharmaceutical drugs, and the effect sizes are, in several cases, more favorable.
SSRIs, by contrast, are built on a mechanism the evidence does not support, produce clinical benefits that are marginal at best in the populations most commonly prescribed them, and carry a side-effect profile that is rarely communicated honestly.

When a nutrient reduces depressive symptoms, this does not indicate that it has drug-like properties. It indicates that its absence was producing pathology. These are not treatments in the way an SSRI is a treatment. They are the removal of conditions that should not have been present.
Depression, in most cases, reflects a biological system operating below the threshold required for normal function. The brain is a nutrient-dependent organ, and its capacity to regulate mood is directly contingent on the inputs it receives.
No single nutrient should be treated as a cure. The effect sizes here come from isolating one variable in a trial, but depression rarely has one cause and rarely resolves through one input. Correcting a single deficiency may help, but the more reliable approach would be to meet your nutrient requirements comprehensively.
A nutrient-dense diet supplies these compounds together and—paired with adequate sleep, daylight, and movement—produces better outcomes than any single nutrient on its own. Across these interventions, the evidence points to results that meet or exceed SSRIs, with far fewer side effects and the underlying cause corrected.
[1] Elgaddal et al. (2025), Characteristics of Adults Age 18 and Older Who Took Prescription Medication for Depression: United States, 2023
[2] Moncrieff et al. (2022), The serotonin theory of depression: a systematic umbrella review of the evidence
[3] Noetel et al. (2024), Effect of exercise for depression: systematic review and network meta-analysis of randomised controlled trials
[4] Chang et al. (2025), Resistance training for depression: a systematic review and meta-analysis of randomized controlled trials
[5] Wang et al. (2025), Impact of combined aerobic and resistance training on depression: a systematic review and meta-analysis of randomized controlled trials
[6] Menegaz et al. (2025), Bright light therapy for nonseasonal depressive disorders: a systematic review and meta-analysis
[7] Tong et al. (2024), The effect of bright light therapy on major depressive disorder: a systematic review and meta-analysis of randomized controlled trials
[8] Shafiee et al. (2025), Effect of saffron versus selective serotonin reuptake inhibitors (SSRIs) in treatment of depression and anxiety: a meta-analysis of randomized controlled trials
[9] Ghaemi et al. (2024), The effect of vitamin D supplementation on depression: a systematic review and dose-response meta-analysis of randomized controlled trials
[10] Moabedi et al. (2023), Magnesium supplementation beneficially affects depression in adults with depressive disorder: a systematic review and meta-analysis of randomized clinical trials
[11] Swardfager et al. (2013), Zinc in depression: a meta-analysis
[12] Yosaee et al. (2022), Zinc in depression: from development to treatment: a comparative/dose response meta-analysis of observational studies and randomized controlled trials
[13] Yasugaki et al. (2025), Bidirectional relationship between sleep and depression
[14] Scheer et al. (1999), Light affects morning salivary cortisol in humans
[15] Luna-Rangel et al. (2025), Efficacy of blue-light blocking glasses on actigraphic sleep outcomes: a systematic review and meta-analysis of randomized controlled crossover trials
[16] Cotter et al. (2025), Examining the effect of L-theanine on sleep: a systematic review of dietary supplementation trials
[17] Bannai et al. (2012), New therapeutic strategy for amino acid medicine: glycine improves the quality of sleep
[18] Kramer et al. (2024), Apigenin: a natural molecule at the intersection of sleep and aging